If you search "peptides for low testosterone," you will find a dense market of injectable compounds, grey-market clinics, and podcast segments that blur several distinct categories of medicine together in ways that are, charitably, confusing — and, less charitably, misleading. The two most important facts are not buried in fine print: testosterone is a steroid hormone, not a peptide, and the growth hormone-releasing peptides that dominate most "low T peptide" marketing do not raise testosterone in men with genuine hypogonadism. Understanding what separates these categories is the only way to evaluate what has actual evidence, what the American Urological Association recommends for confirmed testosterone deficiency, and which legitimate peptide-class medications — not grey-market injectables — do play a real, FDA-relevant role in the clinical picture (what-are-peptides, peptides-for-men-over-40).
Summary / Quick Answer
Testosterone is a steroid hormone. It is not a peptide. No peptide supplement sold over the counter raises testosterone to clinically meaningful levels in men with diagnosed hypogonadism. The growth hormone-releasing peptides (GHRPs) most heavily marketed for low T — CJC-1295, ipamorelin, sermorelin — affect the GH/IGF-1 axis only, not the hypothalamic-pituitary-gonadal (HPG) axis that governs testosterone production. Two legitimate peptide-class or peptide-adjacent molecules do appear in the clinical hypogonadism literature with real evidence: gonadorelin (synthetic GnRH, a decapeptide) and human chorionic gonadotropin (HCG, a glycoprotein composed of peptide subunits). Both require a physician prescription and a confirmed diagnosis.
The AUA diagnostic threshold for hypogonadism is two early-morning total testosterone measurements below 300 ng/dL, combined with symptoms (PMID 29601923). Lab work comes first. If that threshold is met, the standard of care is physician-supervised testosterone replacement therapy — not peptides marketed online.
Best path if you suspect low T:
- Get a morning serum total testosterone panel on two separate occasions
- Evaluate symptoms with a physician (reduced libido, erectile dysfunction, fatigue, reduced muscle mass)
- If confirmed, discuss FDA-approved TRT options — gel, injection, or pellet — which are testosterone, not peptides
- If fertility preservation matters, ask about HCG or clomiphene citrate as adjuncts or alternatives
- Avoid self-treating with grey-market GHRPs — they do not correct testosterone deficiency
Why This Gets Searched: The Marketing Problem
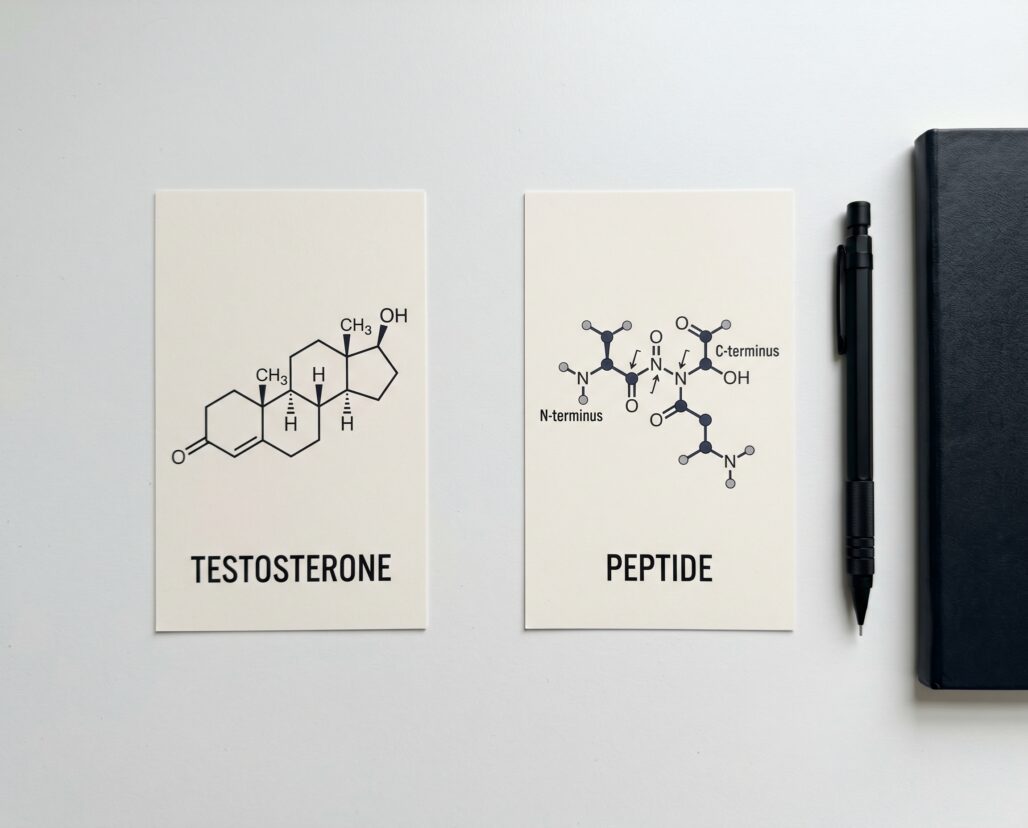
The phrase "peptides for low testosterone" exists because supplement marketers apply the word "peptide" broadly enough to cover almost any molecule they want to promote. Peptide is technically defined as a chain of amino acids linked by peptide bonds, typically fewer than 50 residues before the molecule is classified as a protein. Testosterone does not meet that definition by any stretch. It is a 17-carbon steroid synthesized in the Leydig cells of the testes from cholesterol. It has no amino acid residues. It is not a chain. It does not work through peptide receptors.
The confusion is reinforced by a second layer of conflation: clinics offering growth hormone-releasing peptide protocols position those injections as a "hormonal optimization" package, sometimes bundled with actual testosterone therapy. When a man reads that his clinic is giving him "peptides for hormonal optimization," he may reasonably infer that peptides are doing something to his testosterone. In the majority of GHRP-only protocols, they are not.
Understanding why GHRPs miss the target for low T requires a brief detour into the two separate hormonal axes at play.
Testosterone Is Not a Peptide: The Biology That Matters
Testosterone is produced through a well-characterized cascade. The hypothalamus releases gonadotropin-releasing hormone (GnRH), a decapeptide — that is actually a peptide. GnRH signals the pituitary to release luteinizing hormone (LH), a glycoprotein. LH travels to the Leydig cells in the testes and triggers testosterone synthesis from cholesterol via a series of enzymatic steps.
Testosterone itself is the product of that cascade. It is a steroid molecule — lipid-soluble, derived from cholesterol, and structurally nothing like a peptide. Its effects are mediated by the androgen receptor, a nuclear receptor that works inside cells by binding directly to DNA, a mechanism entirely different from the membrane-bound receptors that most peptides use.
This distinction matters clinically because:
- No amount of peptide supplementation replaces the steroid itself if Leydig cells are not producing adequate testosterone (primary hypogonadism) or if pituitary/hypothalamic signaling is deficient (secondary hypogonadism).
- The two types of hypogonadism require different interventions, and the distinction determines which agents — including which peptide-adjacent drugs — are appropriate.
- Calling testosterone a peptide, or implying that peptides raise testosterone, creates false expectations that delay real treatment.
What Grey-Market Clinics Push — and Why It Misses the Target
CJC-1295, ipamorelin, and sermorelin are the three peptides most commonly sold alongside "low T" messaging. All three operate on the growth hormone axis, not the testosterone axis.
CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH). A 2006 randomized trial in healthy adults found that a single subcutaneous injection produced dose-dependent increases in mean plasma GH concentrations of 2- to 10-fold lasting six days or more, and elevated IGF-I levels 1.5- to 3-fold lasting up to 11 days (PMID 16352683). The study measured FSH, LH, and other pituitary hormones. CJC-1295 did not affect them. It had no measurable effect on the gonadal axis.
Ipamorelin is a synthetic pentapeptide that acts through the ghrelin/GHRP receptor to stimulate GH release. The foundational selectivity study (PMID 9849822) found: "None of the GH secretagogues tested affected FSH, LH, PRL or TSH plasma levels." Ipamorelin is described in its original characterization as the first selective GH secretagogue precisely because it stimulates GH and nothing else in the pituitary panel. It does not stimulate LH. It does not raise testosterone.
Sermorelin is a synthetic GHRH fragment (the first 29 amino acids of native GHRH). Its mechanism is identical to CJC-1295 in principle — it stimulates pituitary somatotrophs to release GH. Like CJC-1295 and ipamorelin, it has no established pathway for raising testosterone.
A 2020 review on growth hormone secretagogues in hypogonadal men (PMID 32257855) examined whether GH secretagogues could address some of the body composition symptoms associated with low T — fat gain, muscle loss — and found that while GH/IGF-1 axis stimulation could improve those parameters, this was distinct from correcting testosterone deficiency. The authors were explicit: GHRPs are adjunctive tools for specific body composition complaints, not replacements for HPG axis management.
The practical bottom line: if your testosterone is low because your HPG axis is not functioning correctly, no amount of CJC-1295, ipamorelin, or sermorelin will correct that. These peptides do not signal the pituitary to release LH, they do not stimulate the testes to produce testosterone, and they do not address the underlying pathophysiology of either primary or secondary hypogonadism.
An additional warning: CJC-1295 and ipamorelin are not FDA-approved for human use in the United States. They are sold by compounding pharmacies and grey-market research suppliers in a regulatory grey area that has narrowed significantly since the FDA reclassified several bulk drug substances in 2023 and 2024. Men self-treating with these compounds have no pharmaceutical-grade quality assurance, no physician monitoring, and no data from long-term human safety trials.
The Legitimate Peptide Options: HCG and Gonadorelin
Two compounds that do work through the testosterone production pathway deserve attention because they are genuinely peptide-class molecules with real clinical evidence and established regulatory status.
Human Chorionic Gonadotropin (HCG)
HCG is a glycoprotein composed of alpha and beta subunit peptide chains. Structurally it belongs to the same hormone family as LH, and at the receptor level it acts as an LH mimetic — binding the same testicular LH receptor and triggering the same testosterone synthesis cascade. Because HCG works downstream in the same pathway that LH uses, it can stimulate testosterone production in men with secondary hypogonadism (where the problem is insufficient pituitary LH output, not a failed testis).
A 2021 narrative review (PMID 33345656) synthesizing literature from 1977-2020 found HCG treatment viable for secondary hypogonadism with two significant advantages over exogenous testosterone: it does not suppress intratesticular testosterone production (which conventional TRT does via negative feedback), and it preserves spermatogenesis, making it the preferred approach for men with hypogonadism who want to maintain fertility. The AUA testosterone deficiency guideline (PMID 29601923) explicitly lists HCG as an option: "Clinicians may use aromatase inhibitors, human chorionic gonadotropin, selective estrogen receptor modulators, or a combination thereof in men with testosterone deficiency desiring to maintain fertility."
HCG is FDA-approved for use in males in specific indications including hypogonadotropic hypogonadism and is available through 503b-compounding pharmacies for clinical hypogonadism management. It is a prescription medication requiring physician oversight and confirmed diagnosis — not an over-the-counter supplement.
Gonadorelin
Gonadorelin is the synthetic form of native GnRH. It is a decapeptide — ten amino acids: 5-oxoPro-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2 — making it a true small peptide by any biochemical definition. It acts at the pituitary level to stimulate LH and FSH release, which then drives testosterone synthesis. In men with hypothalamic hypogonadism — where the hypothalamus fails to produce adequate endogenous GnRH — pulsatile gonadorelin delivery can restore the entire HPG cascade from the top.
A 2019 study in men with congenital hypogonadotropic hypogonadism (PMID 30569789) found that pulsatile gonadorelin pump therapy induced spermatogenesis in a median of 6 months compared to 14 months for cyclical gonadotropin therapy, demonstrating that restoring the upstream GnRH signal can be more physiologically efficient than replacing downstream gonadotropins.
Gonadorelin is FDA-regulated, though its primary approved veterinary indication (under trade names like Cystorelin and Factrel) differs from human use. In human medicine, pulsatile GnRH therapy for hypothalamic hypogonadism has a long clinical literature, though it remains a specialist intervention. Some compounding pharmacies supply gonadorelin for men on TRT who want to maintain testicular function and endogenous testosterone signaling alongside exogenous testosterone — a use case where it functions similarly to HCG but operates one step higher in the axis.
The key point: gonadorelin is a real peptide that does interact with the testosterone production pathway in a medically meaningful way. It is not a grey-market GHRP. It is not a growth hormone secretagogue. And it requires a diagnosed indication, a prescribing physician, and appropriate monitoring.
What the AUA Actually Recommends for Low T
The 2018 AUA Evaluation and Management of Testosterone Deficiency guideline (PMID 29601923) sets the diagnostic and treatment standard that endocrinologists and urologists follow. The criteria are precise and worth knowing because grey-market clinics frequently offer testosterone or testosterone-adjacent compounds to men who do not meet them.
Diagnosis requires:
- At least two early-morning total testosterone measurements below 300 ng/dL
- Measurements taken on separate occasions
- The presence of symptoms and/or signs consistent with testosterone deficiency
- Both biochemical and clinical criteria must be met — low labs alone are not sufficient
Symptoms that most reliably correlate with biochemically confirmed hypogonadism are sexual in nature: reduced morning erections, decreased frequency of sexual thoughts, and erectile dysfunction. General fatigue and muscle loss have many causes and are less specific.
Recommended treatment options include:
- Testosterone gels and transdermal preparations — applied daily, achieve stable levels, require care around transfer to partners or children
- Intramuscular or subcutaneous testosterone injections — cypionate or enanthate, typically every 1-2 weeks; produce levels that peak and trough between injections
- Testosterone pellets — subcutaneously implanted, release testosterone over 3-6 months
All three delivery methods are delivering testosterone — the steroid hormone. None of them are peptide therapies.
The guideline also lists fertility-preserving alternatives including HCG and selective estrogen receptor modulators (SERMs) for men who want to maintain sperm production.
Clomiphene citrate (a SERM, not a peptide) stimulates endogenous testosterone by blocking estrogen's negative feedback on the hypothalamus and pituitary, thereby increasing LH and FSH secretion. A 2022 systematic review and meta-analysis of 19 studies (1,642 patients) found that total testosterone increased by 2.60 nmol/L on average during clomiphene treatment, with concurrent rises in LH, FSH, and free testosterone (PMID 34933414). Side effects occurred in fewer than 10% of patients and no serious adverse events were reported. Clomiphene is not a peptide, but it illustrates that there are alternatives to exogenous TRT that work through the HPG axis upstream — the same territory where HCG and gonadorelin operate.
Frequently Asked Questions
Can peptides raise testosterone?
Not in any clinically meaningful way for men with diagnosed hypogonadism. The grey-market GHRPs (CJC-1295, ipamorelin, sermorelin) operate on the GH/IGF-1 axis and have been explicitly shown not to affect LH or testosterone. HCG and gonadorelin are peptide-class molecules that do interact with the testosterone pathway, but they are prescription medications requiring a confirmed diagnosis — not peptide supplements.
Is testosterone a peptide hormone?
No. Testosterone is a steroid hormone derived from cholesterol. Peptide hormones are made from amino acid chains. Testosterone has no amino acid residues. The distinction is fundamental to understanding why GHRP supplements cannot replace TRT.
What are the symptoms of low testosterone?
The AUA guideline identifies the most diagnostically specific symptoms as reduced morning erections, decreased frequency of sexual thoughts, and erectile dysfunction. General fatigue and decreased muscle mass are also associated with hypogonadism but are less specific because they have many other causes. A confirmed diagnosis requires lab work, not symptom assessment alone.
What is the threshold for diagnosing hypogonadism?
The AUA guideline sets total testosterone below 300 ng/dL on two separate early-morning blood draws as the diagnostic threshold, combined with symptoms. Some endocrinologists use slightly different thresholds, but 300 ng/dL on morning samples is the standard reference point in US clinical practice.
Is HCG a peptide?
HCG is a glycoprotein hormone composed of two peptide subunit chains (alpha and beta). It is technically a peptide-class molecule and is the most evidence-supported peptide-related option for secondary hypogonadism. It is a prescription medication, not a supplement.
Can I self-treat low T with grey-market peptides?
No. This carries multiple risks: CJC-1295 and ipamorelin do not treat testosterone deficiency; grey-market products have no pharmaceutical-grade quality assurance; and the underlying cause of low testosterone requires diagnosis and appropriate management. Self-treating delays real care and may mask symptoms that require investigation.
What about sermorelin for low T?
Sermorelin is a GHRH analog that stimulates GH release. Like CJC-1295 and ipamorelin, it does not raise testosterone and does not address hypogonadism. It is sometimes used by anti-aging clinics as part of broader "hormonal optimization" protocols, but it should not be represented — and is not supported by evidence — as a treatment for confirmed testosterone deficiency.
Conclusion
The peptide landscape for low testosterone is genuinely complicated by poor marketing language, but the underlying biology is not ambiguous. Testosterone is a steroid hormone, not a peptide. The growth hormone-releasing peptides marketed most aggressively for low T — CJC-1295, ipamorelin, sermorelin — act on the GH/IGF-1 axis and do not correct hypogonadism. The two peptide-class molecules that do legitimately appear in the clinical management of low testosterone are HCG (a glycoprotein composed of peptide subunits, FDA-approved for certain hypogonadism indications) and gonadorelin (a synthetic GnRH decapeptide that restores the hypothalamic signal). Both require a physician, a confirmed diagnosis, and appropriate monitoring.
If you are experiencing symptoms that suggest low testosterone, the correct first step is two early-morning total testosterone blood draws — not a peptide protocol. If those results confirm testosterone below 300 ng/dL alongside symptoms, the AUA-supported treatment path is physician-supervised TRT or, for men preserving fertility, HCG or clomiphene citrate. That path involves real medicine, real monitoring, and real accountability — which is what a condition affecting this many physiological systems actually requires.
For related reading, see cjc-1295-explained for a detailed look at what CJC-1295 actually does and does not do, and peptides-for-libido for evidence on compounds with sexual health data.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
