If you have a thyroid condition and a doctor is discussing GLP-1 medications with you, two completely different conversations can happen, and which one you need depends on what kind of thyroid condition you have. If your thyroid diagnosis is Hashimoto's thyroiditis or garden-variety hypothyroidism, you are not looking at a contraindication — you are looking at a drug class that requires some extra monitoring steps and an honest discussion about how delayed gastric emptying can change the way your levothyroxine behaves. If your personal or family history includes medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN-2), the conversation is shorter and firmer: GLP-1 receptor agonists are contraindicated for you, full stop, per every FDA-approved label in the class. Conflating these two situations is one of the more consequential errors that circulates in patient forums, and this guide exists to pull them apart clearly.
Summary: Which Thyroid Situation Are You Actually In?
Before going deeper, the key distinctions in one place:
| Thyroid Situation | GLP-1 Status | Primary Concern |
|---|---|---|
| Hypothyroidism (autoimmune or non-autoimmune), Hashimoto's | NOT contraindicated | Levothyroxine absorption + TSH drift; monitoring needed |
| Personal history of medullary thyroid carcinoma (MTC) | CONTRAINDICATED — absolute | Boxed warning; FDA label; not a risk-benefit conversation |
| Family history of MTC in first-degree relative | CONTRAINDICATED — absolute | Same boxed warning language |
| Multiple Endocrine Neoplasia syndrome type 2 (MEN-2) | CONTRAINDICATED — absolute | Same boxed warning language |
| Papillary or follicular thyroid cancer history | No specific GLP-1 contraindication | Discuss with endocrinologist; these are different cell types than MTC |
| No thyroid history | General population risk; boxed warning is still relevant | Understand the warning before starting |
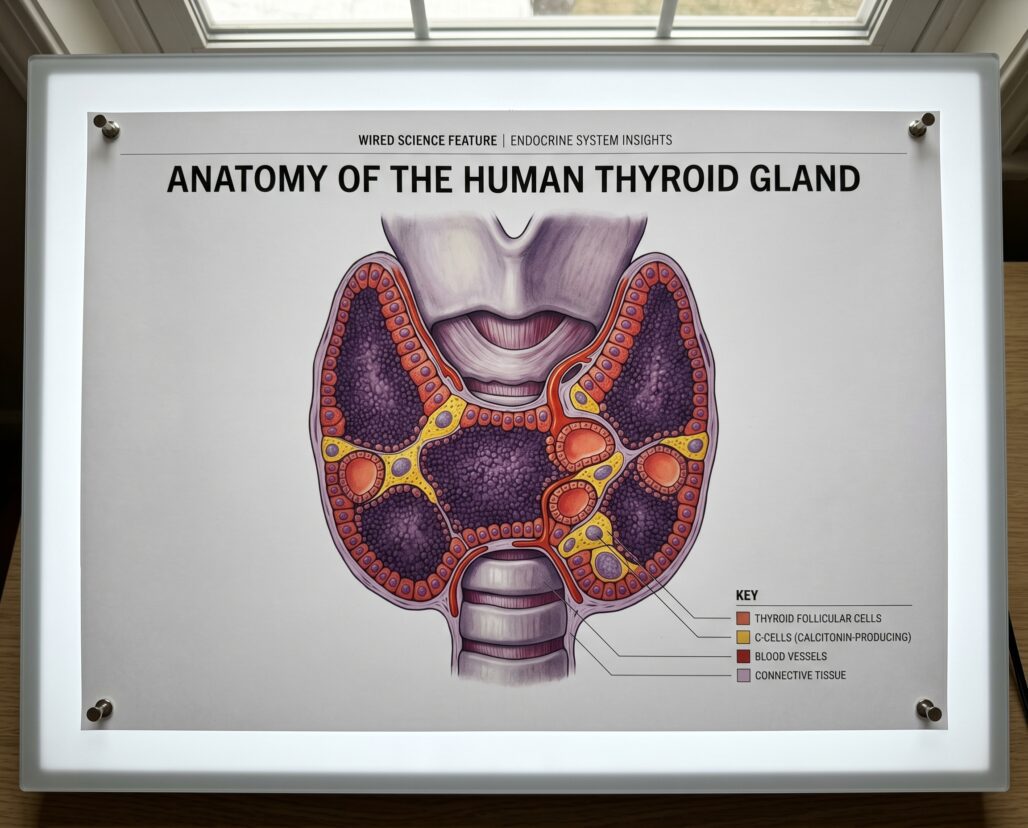
Medullary thyroid carcinoma arises from parafollicular C-cells, which is an entirely different cell lineage from papillary or follicular thyroid cancers. The GLP-1 thyroid concern is specifically about C-cells and only about C-cells. That distinction matters clinically and is poorly understood in most patient-facing coverage of this topic.
The Boxed Warning Explained
A boxed warning is the FDA's highest-tier safety alert, printed in a black border at the top of every prescribing information document. Every GLP-1 receptor agonist on the US market — semaglutide (Ozempic, Wegovy, Rybelsus), liraglutide (Victoza, Saxenda), dulaglutide (Trulicity), exenatide (Byetta, Bydureon), and tirzepatide (Mounjaro, Zepbound) — carries a version of the same warning.
The DailyMed label for Ozempic and Rybelsus states verbatim:
"In rodents, semaglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. It is unknown whether RYBELSUS and OZEMPIC tablets cause thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans as human relevance of semaglutide-induced rodent thyroid C-cell tumors has not been determined."
The animal findings are reproducible and occurred at plasma exposures humans reach during treatment: C-cell hyperplasia, adenomas, and carcinomas in a dose-dependent and duration-dependent pattern across rat and mouse studies. The human relevance is genuinely uncertain because GLP-1 receptors are expressed at much higher density on rodent thyroid C-cells than human ones — that molecular difference is why FDA concluded the human signal is "not determined" rather than confirmed or cleared. "Unknown" in regulatory language is not the same as "probably fine," and FDA has applied this warning consistently to every GLP-1 approval since liraglutide in 2010.
MEN-2 and Family MTC History: The Absolute Contraindication
The contraindication in the Ozempic/Rybelsus prescribing information is unambiguous: "RYBELSUS and OZEMPIC tablets are contraindicated in patients with: A personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)."
The same language, applied to the same patient populations, appears in the prescribing information for tirzepatide (Mounjaro/Zepbound), liraglutide, and every other approved GLP-1 agonist.
This is an absolute contraindication — it does not say "use with caution" or invite a risk-benefit discussion. Contraindicated means do not use. Family history is sufficient to trigger it because MTC is hereditary in approximately 25% of cases, driven by germline RET proto-oncogene mutations in MEN-2A, MEN-2B, and Familial MTC. If a first-degree relative had MTC, the probability of carrying a relevant mutation is high enough that FDA determined the risk of GLP-1 exposure should not be accepted. Genetic counseling and RET testing are the appropriate next step — not starting a GLP-1 agonist while mutation status is unknown.
If you are uncertain whether a family member's thyroid cancer was medullary or papillary/follicular, resolve that question before starting a GLP-1. Medical records, pathology reports, or a genetic counselor can clarify it, and the answer determines whether the contraindication applies to you at all.
Hashimoto's and GLP-1 Agonists: A Completely Different Question
Hashimoto's thyroiditis is an autoimmune condition in which the immune system attacks thyroid follicular cells — the cells that produce T3 and T4. It is the most common cause of hypothyroidism in iodine-sufficient countries. It has nothing to do with thyroid C-cells.
Hashimoto's does not increase MTC risk. It is not associated with MEN-2. It does not make GLP-1 receptor signaling in the thyroid more dangerous. Patients with Hashimoto's hypothyroidism who meet other clinical criteria for GLP-1 therapy — obesity, type 2 diabetes, or cardiovascular risk reduction — are not contraindicated from using GLP-1 agonists. This point has been confirmed in both the American Thyroid Association's clinical guidance and in the FDA labeling itself, which lists only MTC history and MEN-2 as contraindications.
The confusion in patient communities comes from two sources: patients searching "GLP-1 thyroid warning" encountering boxed warning language without parsing which thyroid conditions it covers, and some prescribers blanket-excluding all thyroid patients out of excessive caution. Neither reflects the actual contraindication framework. What Hashimoto's patients do need to know is addressed in the next two sections.
Levothyroxine and GLP-1 Agonists: The Absorption Interaction
Hypothyroidism managed with levothyroxine replacement is common, and GLP-1 receptor agonists are increasingly prescribed to patients with comorbid obesity or type 2 diabetes. Those two drugs will coexist in a growing number of patients, and the interaction is real and important.
GLP-1 receptor agonists slow gastric emptying. That is partly how they reduce appetite — food moves more slowly from the stomach to the small intestine, extending satiety. Levothyroxine is absorbed primarily in the small intestine, and absorption is sensitive to gastric transit time and the presence of food or other substances in the gut. Delayed gastric emptying caused by GLP-1 agonists can alter both the rate and potentially the extent of levothyroxine absorption.
The semaglutide prescribing information documents this directly in its drug interaction section (Section 12.3): "Levothyroxine exposure was increased 33% (90% CI: 1.25 to 1.42) when administered with semaglutide tablets." The mechanism under study is altered gastric emptying kinetics changing how the drug is absorbed and when it reaches peak plasma concentration.
Clinical case data reinforces the importance of monitoring. A 2024 case report (PMID: 38992739, Journal of the American Pharmacists Association) documented a post-thyroidectomy patient who had been stable on levothyroxine for five years before initiating subcutaneous semaglutide. Following semaglutide titration, TSH became suppressed, requiring a 25% dose reduction of levothyroxine. The authors identified three plausible mechanisms: direct GLP-1 receptor effects on TSH secretion, delayed gastric emptying altering levothyroxine absorption, and weight loss reducing the volume of distribution for levothyroxine. All three may have contributed simultaneously.
A 2025 study (PMID: 41444586, Cardiovascular Diabetology) examining older adults on levothyroxine who started GLP-1 therapy found that weight loss added a second, slower mechanism — as body mass decreases, required levothyroxine dose may decrease as well.
The practical implication: TSH should be rechecked within 6-8 weeks of initiating or up-titrating a GLP-1 if you take levothyroxine. Symptoms of over-replacement (palpitations, anxiety, poor sleep) or under-replacement (fatigue, cold sensitivity) after GLP-1 initiation should trigger early testing. Also review levothyroxine administration timing with your prescriber — standard guidance is to take it on an empty stomach, 30-60 minutes before eating, and that matters more when gastric motility is altered.
Calcitonin Monitoring: What the FDA Actually Recommends
Calcitonin is a hormone secreted by thyroid C-cells and serves as a tumor marker for medullary thyroid carcinoma. Some clinicians, particularly outside the United States, order baseline and periodic serum calcitonin measurements in patients starting GLP-1 agonists, on the premise that early C-cell changes might be detectable before clinical MTC develops.
The FDA does not endorse this practice for the general GLP-1 population, and the prescribing information explains why. The Ozempic/Rybelsus label states: "Routine monitoring of serum calcitonin or using thyroid ultrasound is of uncertain value for early detection of MTC in patients treated with RYBELSUS or OZEMPIC tablets." The label further notes that significantly elevated calcitonin values above 50 ng/L may warrant further evaluation, but this is guidance on interpreting abnormal findings rather than a recommendation for universal screening.
Mild calcitonin elevations are common in the general population and can be caused by chronic kidney disease, thyroid goiter, smoking, obesity, and proton pump inhibitor use — among others. Routine calcitonin screening in low-risk GLP-1 users produces anxiety, additional testing, and cost without established evidence of MTC mortality benefit. In patients with MEN-2 or hereditary MTC risk, calcitonin monitoring is appropriate under endocrinology supervision — but those patients should not be on GLP-1 agonists at all.
A baseline calcitonin before starting a GLP-1 is a defensible clinical choice. Ongoing routine monitoring is not FDA-recommended for low-risk patients, and a mildly elevated result in isolation does not confirm a problem.
What Human Observational Data Shows — and Where It Falls Short
The most-cited study in this space is a French nested case-control analysis by Bezin et al. (PMID: 36356111, Diabetes Care, 2023), which matched 2,562 thyroid cancer cases to 45,184 controls in the French national health insurance database. GLP-1 use for 1-3 years was associated with an adjusted hazard ratio of 1.58 (95% CI 1.27-1.95) for all thyroid cancers and 1.78 (95% CI 1.04-3.05) for medullary thyroid cancer. The MTC finding attracted significant attention.
Context matters. MTC affects roughly 1,000 Americans per year — a hazard ratio of 1.78 on that baseline produces a very small absolute risk increase. The MTC confidence interval barely clears 1.0 at its lower bound, and multiple methodological critiques cited confounding by indication, surveillance bias in GLP-1 users, and incomplete adjustment for diabetes duration.
Larger and more recent data has not confirmed the signal. An international cohort study (PMID: 39772758, Thyroid, 2025, Baxter et al.) pooled 98,147 GLP-1 users and over 2.4 million DPP-4 inhibitor comparators across Canada, Denmark, Norway, South Korea, Sweden, and Taiwan. The pooled hazard ratio for thyroid cancer was 0.81 (95% CI 0.59-1.12) — no elevated risk and no dose-response relationship. A Korean cohort (PMID: 37735822, 2024, Bea et al.) using 21,722 GLP-1 users versus SGLT2 inhibitor controls found a hazard ratio of 0.98 (95% CI 0.62-1.53), essentially null on both all thyroid cancers and MTC subgroup.
The honest read: the French study raised a signal; the larger and more recent data has not confirmed it. None of the studies have follow-up long enough to rule out long-latency effects. FDA has not changed the boxed warning or added new monitoring requirements. The contraindications remain unchanged.

Frequently Asked Questions
I have Hashimoto's and my doctor wants to prescribe Ozempic for weight loss. Should I be worried about the thyroid warning?
The boxed warning applies to medullary thyroid carcinoma risk, which involves thyroid C-cells. Hashimoto's affects follicular cells and is autoimmune in nature. These are unrelated processes. You are not in the contraindicated category unless you also have personal or family history of MTC or MEN-2. What you do need is a TSH recheck 6-8 weeks after starting the GLP-1 if you take levothyroxine, because the drug can alter how your thyroid replacement is absorbed and metabolized.
I found out that my aunt had "thyroid cancer." Does that automatically mean I can't take a GLP-1?
Not automatically — the answer depends on what type of thyroid cancer she had. If it was papillary or follicular thyroid cancer (by far the most common types), the contraindication does not apply to you. If it was medullary thyroid cancer, that is a different situation and you need RET mutation genetic testing and endocrinology consultation before starting a GLP-1 agonist. Get the pathology type confirmed before drawing any conclusions.
I've been reading about compounded semaglutide. Does it have the same thyroid risks?
FDA has issued explicit cautions about compounded GLP-1 medications. Beyond quality, potency, and sterility concerns with compounded products, any compound that contains semaglutide or a functionally similar GLP-1 agonist carries the same mechanistic risk profile as the branded drug. The thyroid C-cell concern arises from the pharmacology of GLP-1 receptor activation, not from a specific formulation. The contraindications for MTC history and MEN-2 apply regardless of whether the drug comes from a licensed pharmacy or a compounding facility.
I'm pregnant and taking a GLP-1 for diabetes. What should I know?
GLP-1 receptor agonists should be discontinued before conception or as soon as pregnancy is detected. All FDA-approved GLP-1 labels state the drugs should not be used during pregnancy — weight loss is not appropriate during pregnancy, and human developmental safety data is insufficient. Semaglutide's half-life is approximately one week with extended tissue effects, so discontinuing several months before attempting to conceive is standard guidance. Discuss the transition plan with your prescriber well in advance.
My calcitonin came back slightly elevated. Do I need to stop my GLP-1?
A mildly elevated calcitonin result requires interpretation in full clinical context, not an automatic stop. Calcitonin can be elevated by many causes unrelated to thyroid disease. Your prescriber will likely want to repeat the test, assess other potential causes, and potentially refer to endocrinology if values are significantly elevated (the FDA label notes values above 50 ng/L warrant further evaluation). Do not stop a prescribed medication based on a single lab result without discussing it with your doctor first.
Conclusion
The thyroid and GLP-1 story has two chapters that bear almost no resemblance to each other. Chapter one is the boxed warning: real rodent carcinogenicity data, a mechanistically plausible C-cell pathway, an absolute contraindication for anyone with MEN-2 or personal or family history of medullary thyroid carcinoma, and human population data that has so far been largely reassuring while remaining too short-term to close the question definitively. Chapter two is hypothyroidism and Hashimoto's: no contraindication, a meaningful but manageable drug interaction with levothyroxine, and a monitoring plan that any attentive prescriber can implement.
The error — and it happens with real clinical consequences — is treating chapter two as if it were chapter one. Patients with Hashimoto's who would benefit from GLP-1 therapy being excluded based on a boxed warning that does not apply to them. Patients with actual family MTC history being started on a GLP-1 because their prescriber did not take a careful enough thyroid cancer family history. Both errors are avoidable with the same tool: precise diagnosis of which thyroid situation you are actually in, verified before a prescription is written.
If you have any thyroid history, bring the pathology type, the family history specifics, and your current medication list (especially levothyroxine) to the appointment where GLP-1 therapy is being considered. Those details determine which chapter applies to you.
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The information presented here is based on publicly available research and FDA-approved prescribing information as of the publication date and may not reflect subsequent updates. Always consult a qualified healthcare provider — including your prescribing physician and, where appropriate, an endocrinologist — before starting, stopping, or adjusting any prescription medication. If you have a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2, discuss this explicitly with your doctor before any GLP-1 agonist is prescribed.
