Scroll the comments on any hair-growth post and you will find someone asking whether copper peptide serums actually work, or whether they are just expensive window dressing. The skepticism is fair. The hair loss supplement market runs on hope, and brands have learned to dress up ingredient lists to sound clinical. So here is the honest version: peptides for hair loss do have real mechanistic rationale, a handful of small but legitimate human trials back some of them up, and the evidence is promising enough to take seriously. Verdict: peptides, particularly GHK-Cu and biotinyl-tripeptide-1, are a credible adjunct to proven therapies — not a replacement for them.
Summary / Quick Answer: Do Peptides Actually Help With Hair Loss?
Yes, with caveats. Copper peptides (especially GHK-Cu) and multi-peptide complexes like biotinyl-tripeptide-1 have shown measurable hair count improvements in small, controlled human studies. They work through different mechanisms than minoxidil or finasteride, which is why they make sense as add-ons rather than substitutes.
Best for: People with androgenetic alopecia (genetic pattern hair loss) or mild telogen effluvium (stress-related shedding) who want to layer additional actives on top of, or as an alternative when they cannot tolerate, standard treatments.
Not ideal for: Anyone expecting peptide serums to deliver the same density gains as 5% minoxidil used consistently. The evidence gap is real.
What to look for: Products listing GHK-Cu (copper peptide complex), biotinyl-tripeptide-1 (sold under trade names like Capixyl or Baicapil), or multi-complex blends such as Procapil or Redensyl. Concentration matters; most clinical work uses 2–5% active.
Decision shortcut: If you have not yet tried minoxidil and your hair loss is genetic in origin, start there. If you are already on minoxidil and want to add a layer, a well-formulated copper peptide or peptide-complex serum is a reasonable next step based on current evidence.
How Hair Loss Actually Works (The Biology You Need)
Most people experiencing thinning hair have one of two things happening, and they require different thinking.
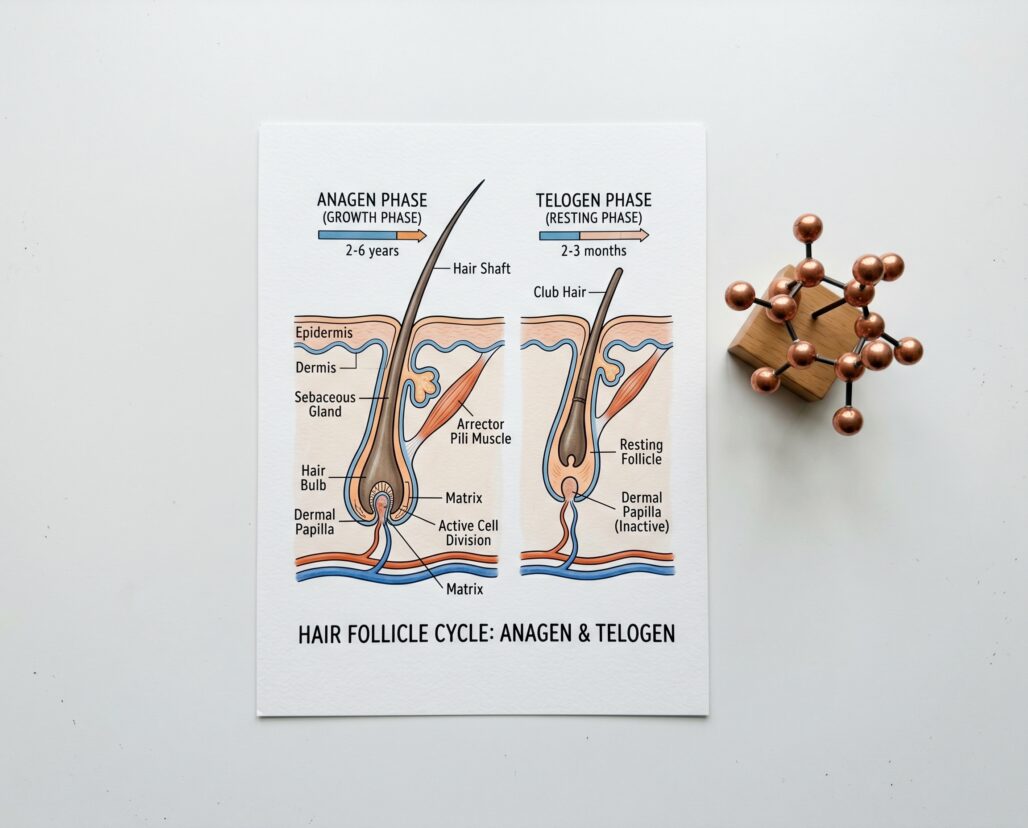
Androgenetic alopecia (AGA) — pattern baldness in men and women — is driven by dihydrotestosterone (DHT). The enzyme 5-alpha reductase converts testosterone to DHT, which then binds androgen receptors in hair follicle dermal papilla cells. In genetically susceptible follicles, this shrinks the anagen (growth) phase progressively shorter with each cycle. Follicles miniaturize, producing thinner and shorter hairs until the follicle eventually stops producing terminal hair altogether. This is the mechanism described in StatPearls' comprehensive AGA review.
Telogen effluvium (TE) is different: a systemic stressor (illness, severe caloric restriction, major surgery, postpartum hormonal shifts) throws a larger-than-normal proportion of follicles into telogen simultaneously, causing diffuse shedding two to four months later. TE is usually self-limiting once the trigger resolves.
Why does this distinction matter for peptides? AGA responds best to treatments that interrupt DHT signaling (finasteride) or extend anagen via other pathways (minoxidil). Peptides that promote follicle cell proliferation and reduce oxidative stress may help both conditions — but they do not block DHT, so they cannot address the upstream driver of AGA on their own.
The Peptides Most Often Claimed for Hair Growth
Three categories dominate the ingredient landscape:
1. GHK-Cu (Glycyl-L-Histidyl-L-Lysine Copper Complex) A naturally occurring tripeptide first identified in human plasma. It chelates copper (II) ions, and that copper-peptide complex is the biologically active form. GHK-Cu has well-documented actions on wound healing and tissue remodelling, and those same mechanisms — stimulating keratinocyte proliferation, increasing collagen synthesis, activating integrin expression — are relevant to follicle health. To understand how GHK-Cu functions at the cellular level, the broader mechanistic context in our copper peptides overview is worth reading before purchasing a serum.
2. Biotinyl-Tripeptide-1 (sold as Capixyl, a blend of biotinyl-tripeptide-1 + red clover extract) A synthetic peptide that mimics the structure of laminin, an adhesion protein in the follicle basement membrane. The proposed mechanism is improved anchoring of the follicle in the dermal matrix and mild inhibition of 5-alpha reductase. Capixyl combines biotinyl-tripeptide-1 with red clover isoflavones for a dual-mechanism approach.
3. Multi-peptide complexes: Redensyl, Procapil, AnaGain These are proprietary blends rather than single peptides. Redensyl targets hair follicle stem cells via DHQG and EGCG2. Procapil combines biotinyl-tripeptide-1 with apigenin and oleanolic acid. AnaGain is a pea sprout (Pisum sativum) extract standardized for growth-factor-stimulating phytoactives. They are common in mid-to-premium retail serums and have their own small clinical datasets.
What the Evidence Actually Shows
This is where the honest accounting matters. Evidence level in order from weakest to strongest: in vitro (cell cultures), animal studies, uncontrolled human observational studies, small randomized controlled trials (RCTs), large RCTs.
GHK-Cu: Promising Small-Scale Human Data
The strongest hair-specific human study tested ALAVAX — a combination of 5-aminolevulinic acid and GHK peptide — in 45 men with male pattern hair loss over 6 months (PMID 27489425). Both active groups showed statistically significant hair count gains versus placebo: +52.6 hairs (higher concentration) and +71.5 hairs (lower concentration), compared to +9.6 in the placebo group. No adverse events were reported. Actionable note: this is the best single human trial for GHK in hair, but the sample is 45 participants using a compound formulation — not a standalone GHK-Cu serum. Earlier in-vitro work from Pyo et al. (2007) showed the copper-tripeptide complex stimulates isolated human hair follicle growth directly, which gives the human finding a plausible cellular mechanism.
The broader GHK-Cu review by Pickart and Margolina (PMC6073405, PMID 29986520) catalogs GHK-Cu's regenerative effects across skin and connective tissue but notes that hair-specific human RCT data remains limited. The in-vitro and in-vivo mechanistic picture is solid; the large-scale clinical picture is not yet there.
Biotinyl-Tripeptide-1 / Capixyl: Combination Evidence Only
No clean, single-ingredient human RCT exists for biotinyl-tripeptide-1 alone. What exists is combination data. A 2023 open-label trial published in Cosmetics (MDPI) tested a topical-plus-oral regimen containing oleanolic acid, apigenin, and biotinyl-tripeptide-1 in patients with AGA and showed a 12.14 hairs/cm2 increase in 3 months with the combined therapy. In vitro, a serum containing biotinoyl-tripeptide-1 reduced 5-alpha reductase expression and increased dermal papilla cell proliferation comparably to minoxidil at matched culture conditions — but in-vitro comparisons do not translate directly to scalp outcomes.
The real question is not whether biotinyl-tripeptide-1 does something, but whether it does enough on its own. Every positive study uses it in a multi-ingredient stack, which makes isolating its contribution impossible.
Multi-Complex Blends: Best Head-to-Head Data
A 2022 PMC review (PMC12251978) synthesized the available topical alternative evidence. The Redensyl + Procapil + Capixyl combination showed significantly higher researcher improvement scores versus 5% minoxidil (64.7% vs 25.5% in one 106-patient study), though the review cautions that most studies have small samples, limited follow-up, and frequent industry sponsorship.
AnaGain (pea sprout extract) has a separate small clinical dataset: a 2019 pilot study (PMID 31680356) in 20 volunteers with mild-to-moderate hair loss applied 4% AnaGain gel twice daily for 3 months and found a significant improvement in the anagen-to-telogen hair ratio. A 2025 mechanistic study confirmed anagen phase prolongation and dual anti-oxidant/anti-inflammatory effects in in vitro and in vivo models.
The pattern across all these ingredients is consistent: evidence level 2 on the Oxford scale (small RCTs or well-designed cohort studies), often in combination formulations, rarely with a placebo arm large enough to draw firm conclusions.
Where Peptides Fit Alongside Minoxidil and Finasteride
Minoxidil and finasteride are the only two treatments the FDA has approved for androgenetic alopecia. That approval status reflects decades of clinical evidence, not just regulatory preference.
Minoxidil (topical 2% and 5%) works by shortening the telogen phase, extending anagen, and stimulating vascular endothelial growth factor in the follicle microenvironment. The StatPearls minoxidil entry (PMID 29494000) notes that the 5% solution provides meaningfully better outcomes than the 2% formulation, and benefits emerge around 8 weeks with peak results at 4 months. Crucially, effects reverse when you stop using it.
Finasteride (oral 1 mg, prescription only for men) blocks 5-alpha reductase types II and III, reducing serum DHT by approximately 70% and scalp DHT by up to 90%. It addresses the root cause of AGA in a way that topicals cannot match. Critical safety note: finasteride is pregnancy category X and is contraindicated in women of childbearing potential. Even handling crushed tablets poses a teratogenicity risk. Finasteride requires a physician conversation before starting — this is non-negotiable.
Peptide hair serums often work alongside, not instead of, the proven options. Their mechanisms are largely complementary: GHK-Cu promotes follicle cell proliferation and matrix integrity; minoxidil extends anagen and improves circulation; finasteride reduces the DHT signal driving miniaturization. None of these mechanisms cancel out the others.
Actionable takeaway: if you have genetic hair loss and have not tried FDA-approved treatments, peptide serums are not the right first move. They are a reasonable layer to add once you have the foundation in place, or for people with telogen effluvium where no DHT-blocking treatment is needed.
For a deeper look at how copper peptides function across different use cases, our peptides for skin article covers the cross-tissue research.
What to Look for When Buying a Peptide Hair Serum
The ingredient list is the only reliable signal in this category. Here is what actually matters at the formulation level:
GHK-Cu concentration. Most credible formulations list copper peptide at 1–3%. Higher is not always better because copper at very high concentrations can be pro-oxidant; the clinical data sits in the low-to-mid percentage range.
Biotinyl-tripeptide-1 or the Capixyl trade name. If a serum markets itself on "peptides for hair" without specifying which ones, treat that as a red flag. The ingredient should appear on the INCI list.
Stability and pH. Peptides degrade in poorly buffered formulas. An acidic, preservative-appropriate formula (pH 4–5 for most peptides) in opaque or dark glass packaging preserves activity significantly better than clear plastic.
Absence of irritants that undermine the scalp barrier. Strong alcohols, fragrance, and aggressive surfactants in leave-on scalp serums can cause the kind of low-grade inflammation that works against follicle health. The simpler the carrier, the better.
Realistic timeline expectations. The clinical studies above used 3–6 month endpoints. Any product promising results in 2–4 weeks is overstating what the science supports.
Legitimate copper peptide is not cheap to manufacture, and a meaningful dose in a stable carrier formula costs money. Serums priced at $8 for a 2 oz bottle are likely underdosed or degraded at the point of sale.

FAQ
Can I use a copper peptide serum and minoxidil at the same time? Yes. They work through different mechanisms, and there is no known interaction. Apply one and wait for it to absorb fully before applying the other. Most protocols recommend spacing them by at least 30 minutes.
Do peptide serums help with telogen effluvium? Possibly. TE is usually self-resolving, so it is hard to credit any topical with the recovery. The follicle-supportive and anti-inflammatory effects of GHK-Cu are plausible supports during recovery, but there is no TE-specific clinical trial for copper peptide serums.
Are there injectable peptides for hair loss I should know about? Grey-market injectable peptides marketed for hair growth (including various growth-hormone-releasing peptides sometimes discussed in bodybuilding forums) are outside the scope of what topical evidence supports and carry real risks related to dosing, contamination, and off-target hormonal effects. This article covers topical applications only, and injectable peptide use for any aesthetic purpose requires medical supervision.
How long before I see results from a peptide hair serum? Based on the available clinical data: 3–6 months of consistent use, minimum. Anagen cycles are slow. Patience is not optional here.
Is there a difference between GHK and GHK-Cu? Yes. GHK (the tripeptide alone) has some activity, but GHK-Cu — the copper-chelated form — is the biologically active molecule studied for follicle effects. Look for the copper-complex specifically on the label.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion: The Bottom Line on Peptides for Hair Loss
Peptides for hair loss are not marketing fiction, but the evidence base is not at the level of minoxidil or finasteride either. GHK-Cu has the most credible human trial data in this category, with the 45-patient, 6-month ALAVAX study showing meaningful hair count gains over placebo. Biotinyl-tripeptide-1 and multi-complex blends like Procapil and Redensyl have smaller, often industry-sponsored data showing benefits — but always in combination formulas.
The evidence standard is clear: peptide serums are adjuncts, not anchors. They are a legitimate addition to a hair-loss protocol once the proven options are in place. For androgenetic alopecia, that means having a conversation with a dermatologist about minoxidil first, and finasteride if appropriate (men only, with full awareness of the contraindications). For telogen effluvium, addressing the triggering stressor matters more than any topical.
Actionable takeaway: choose a serum that lists GHK-Cu or biotinyl-tripeptide-1 specifically, use it for at least 3 months before evaluating results, and layer it with — not in place of — the treatments that have decades of trial evidence behind them.
Next steps:
- Learn how copper peptides behave across different tissues in our copper peptides overview
- Compare peptide mechanisms to other topical actives in our peptides for skin guide
- If you want to understand the foundational science, what are peptides explains the biochemistry without jargon
- Talk to a board-certified dermatologist before starting finasteride or if your hair loss is sudden, patchy, or accompanied by other symptoms
As an Amazon Associate, I earn from qualifying purchases. Product recommendations are based on real reviews and independent research.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
As an Amazon Associate, I earn from qualifying purchases. Product recommendations are based on real reviews and independent research.
