If you have heard about Ozempic or Wegovy in the past few years, you may not realize those drugs belong to a class that has been in clinical use since 2010, built on a molecule called liraglutide. The natural question is whether the original version is still relevant now that once-weekly alternatives dominate the headlines. The honest answer is more nuanced than either enthusiasts or skeptics tend to admit. Liraglutide remains an FDA-approved, extensively trialed prescription drug with a well-characterized safety profile — but once-weekly semaglutide has largely displaced it for new prescriptions, and patients who prefer daily dosing, or who need the specific pediatric indication for adolescents aged 12 and older, still have clinically sound reasons to use it.
Summary
Liraglutide is a once-daily injectable GLP-1 receptor agonist approved by the FDA under two brand names: Victoza (2010, type 2 diabetes) and Saxenda (2014, chronic weight management in adults and adolescents 12 and older). Large randomized trials demonstrate meaningful HbA1c reduction, 5 to 8 percent body weight loss versus placebo, and a significant reduction in cardiovascular death in patients with type 2 diabetes. It is a prescription drug, not a supplement, and it carries a boxed warning about thyroid C-cell tumors.
- Two branded products: Victoza (NDA 022341, FDA approved January 2010, type 2 diabetes) and Saxenda (NDA 206321, FDA approved December 2014, chronic weight management).
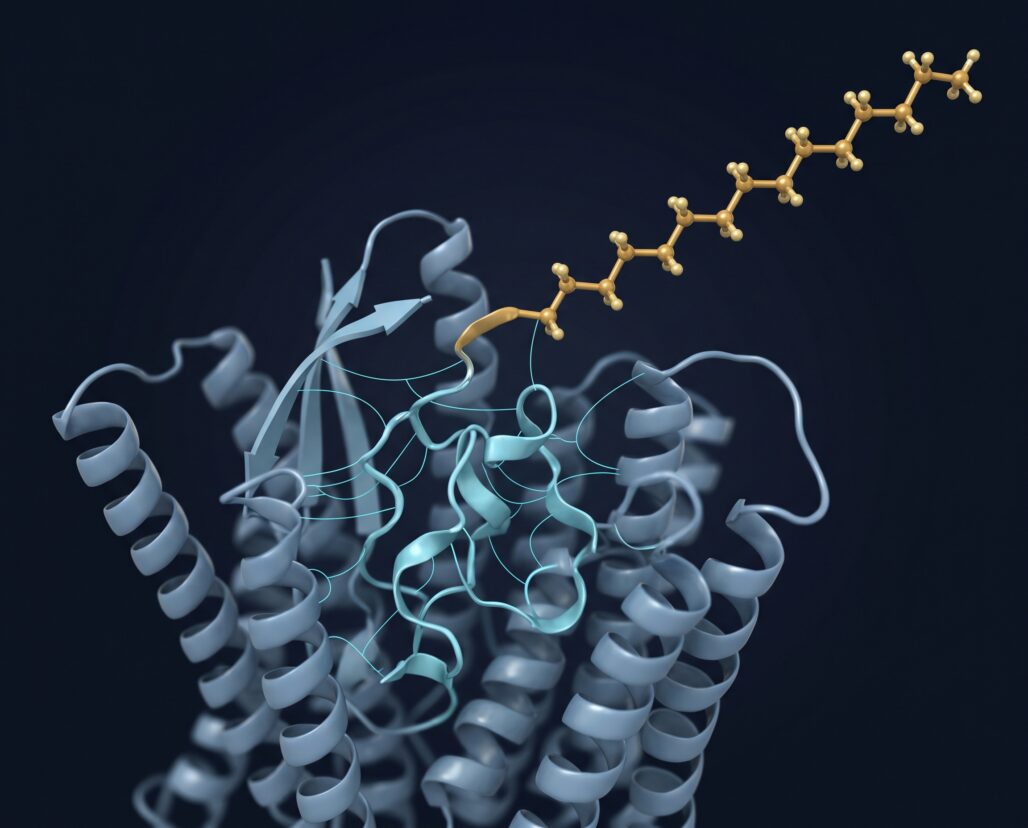
- Pharmacology: 97% amino acid sequence homology with native GLP-1, modified with a C16 fatty acid chain via glutamic acid spacer at position 26 for albumin binding — extending half-life to approximately 13 hours and enabling once-daily subcutaneous dosing.
- SCALE Obesity trial (PMID 26132939): Liraglutide 3 mg produced mean weight loss of 8.4 kg versus 2.8 kg with placebo over 56 weeks in 3,731 adults; 63.2% of liraglutide-treated patients lost at least 5% of body weight compared with 27.1% on placebo.
- SCALE Diabetes trial (PMID 26284720): In adults with type 2 diabetes, liraglutide 3 mg produced 6% weight loss versus 2% with placebo over 56 weeks; 54.3% achieved at least 5% weight loss.
- LEADER cardiovascular trial (PMID 27295427): Among 9,340 adults with type 2 diabetes at high cardiovascular risk, liraglutide reduced the primary three-point MACE composite by 13% (HR 0.87, p=0.01) and cardiovascular mortality by 22% (HR 0.78, p=0.007) over a median 3.8-year follow-up.
- Pediatric indication: Saxenda is the only GLP-1 weight-management drug with an FDA approval specifically for adolescents aged 12 and older with a body weight above 60 kg and obesity. Use must be specialist-supervised.
- Hard limits: Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN-2) is an absolute contraindication. Pancreatitis is a serious known risk.
What Liraglutide Is: Pharmacology and Structure
Glucagon-like peptide-1 (GLP-1) is released by intestinal L-cells after a meal and stimulates glucose-dependent insulin secretion. Native GLP-1 is destroyed by the enzyme DPP-4 within about 90 seconds, making it useless as a drug at physiologic concentrations.
Novo Nordisk solved this by modifying liraglutide at two positions: substituting arginine for lysine at position 34 to block DPP-4 cleavage, and attaching a C16 palmitic acid chain through a glutamic acid spacer at position 26. That fatty acid binds to albumin in plasma, which acts as a depot reservoir. As albumin slowly releases liraglutide, the effective half-life reaches approximately 13 hours — long enough for once-daily dosing. Semaglutide's longer C18 fatty acid chain and additional modification extend its half-life to roughly seven days, which is the pharmacological basis for the once-weekly dosing difference between the two drugs.
Liraglutide is more than 98% protein-bound in plasma, reaches peak concentration approximately 11 hours post-injection, and has a subcutaneous bioavailability of roughly 55%.
For more on how synthetic peptide engineering enables therapeutic stability, see what are peptides and the FDA-approved peptides overview.
Two Branded Products: Victoza and Saxenda
Liraglutide is sold under two brand names with different approved doses and different approved patient populations. They are not interchangeable.
| Brand | Indication | Approved dose | Approval year |
|---|---|---|---|
| Victoza | Type 2 diabetes glycemic control; CV risk reduction in T2D with established CVD | 1.2 mg or 1.8 mg daily SC | 2010 |
| Saxenda | Chronic weight management (adults and adolescents 12+ with obesity; adults with overweight and at least one comorbidity) | 3 mg daily SC (after escalation) | 2014 |
Both products use the same molecule. The practical difference is dose: Victoza tops out at 1.8 mg daily for diabetes management, while Saxenda reaches 3 mg for weight management. Victoza's January 2010 approval made liraglutide the first GLP-1 receptor agonist approved in the United States. Saxenda's 2014 obesity indication was the first time any GLP-1 drug received an obesity label, predating Wegovy by seven years. Using one product off-label as a substitute for the other is not supported by the FDA labeling.
LEADER Cardiovascular Outcomes Trial
The LEADER trial (NCT01179048) enrolled 9,340 adults with type 2 diabetes and either established cardiovascular disease or high cardiovascular risk. Participants were randomized to liraglutide 1.8 mg daily or placebo and followed for a median of 3.8 years. The primary endpoint was the three-point MACE composite: cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. Results, published in the New England Journal of Medicine in 2016 (Marso et al., PMID 27295427):
- Primary MACE: Occurred in 13.0% of the liraglutide group versus 14.9% of the placebo group (HR 0.87; 95% CI 0.78–0.97; p=0.01 for superiority).
- Cardiovascular death: 4.7% with liraglutide versus 6.0% with placebo (HR 0.78; 95% CI 0.66–0.93; p=0.007).
- All-cause mortality: 8.2% versus 9.6% (HR 0.85; 95% CI 0.74–0.97; p=0.02).
- Heart failure hospitalization: No statistically significant difference (HR 0.87; 95% CI 0.73–1.05).
LEADER was the first large randomized trial to show a GLP-1 receptor agonist could reduce cardiovascular death in T2D, not just lower blood sugar. That 22% relative reduction in cardiovascular mortality shaped Victoza's FDA labeling and the clinical logic for preferring liraglutide in higher-risk patients. One caveat: LEADER enrolled a high-risk T2D population, and those cardiovascular benefits should not be assumed to transfer to people using Saxenda for weight management without diabetes.
SCALE Weight-Loss Trial Program
Saxenda's approval rested on the SCALE program (Satiety and Clinical Adiposity — Liraglutide Evidence in Non-diabetic and Diabetic Individuals), a set of randomized trials evaluating liraglutide 3 mg versus placebo as an adjunct to diet and exercise.
SCALE Obesity and Prediabetes (NCT01272219)
The pivotal trial, published in the New England Journal of Medicine in 2015 by Pi-Sunyer et al. (PMID 26132939), enrolled 3,731 adults without diabetes who had a BMI of 30 or greater, or a BMI of at least 27 with at least one weight-related comorbidity. Mean BMI was 38.3. Over 56 weeks:
- Mean weight loss: 8.4 kg with liraglutide versus 2.8 kg with placebo — a difference of 5.6 kg.
- Patients losing at least 5% of body weight: 63.2% (liraglutide) versus 27.1% (placebo).
- Patients losing at least 10% of body weight: 33.1% versus 10.6%.
- Serious adverse events: 6.2% (liraglutide) versus 5.0% (placebo).
- Most common adverse events: nausea and diarrhea, classified as mild to moderate.
For a 100 kg person, 8.4 kg translates to roughly 8.4% of body weight — clinically meaningful for blood pressure, lipids, and glycemic markers, but materially smaller than the 14.9% seen in STEP-1 with semaglutide. The efficacy gap is real and a legitimate factor in shared decision-making.
SCALE Diabetes (NCT01272232)
A parallel SCALE trial (Davies et al., JAMA 2015, PMID 26284720) enrolled 846 adults with type 2 diabetes, a population with typically lower absolute weight-loss response to GLP-1 agents. Over 56 weeks:
- Liraglutide 3 mg: 6.0% weight loss (approximately 6.4 kg) versus 2.0% (approximately 2.2 kg) with placebo.
- At least 5% weight loss: 54.3% versus 21.4%.
- At least 10% weight loss: 25.2% versus 6.7%.
The diabetes population's smaller absolute response underscores that liraglutide is not a uniform-effect drug. Patients with higher insulin resistance or on concomitant insulin typically see less weight loss than those without diabetes.
Pediatric Approval (2020)
In December 2020, the FDA approved Saxenda for adolescents aged 12 and older with a body weight above 60 kg and an initial BMI at or above the 95th percentile for age and sex. This was a separate regulatory action supported by a dedicated pediatric trial. The prescribing information is explicit: use in this age group requires specialist supervision, the dose escalation may extend up to 8 weeks, and patients not tolerating 3 mg may maintain at 2.4 mg. Safety and effectiveness in pediatric type 2 diabetes have not been established for Saxenda.
Side Effects and Safety Warnings
Boxed Warning: Thyroid C-Cell Tumors
Both Victoza and Saxenda carry the same FDA boxed warning. In rodent studies, liraglutide caused dose- and duration-dependent thyroid C-cell adenomas and carcinomas at exposures comparable to clinical levels. Whether this applies to humans is unknown; human thyroid C-cells express very few GLP-1 receptors. The FDA requires the warning because the risk cannot be excluded and medullary thyroid carcinoma is difficult to detect early.
Absolute contraindications: Liraglutide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN-2). These are hard stops, not relative contraindications. Patients should report any neck mass, hoarseness, or persistent difficulty swallowing to their prescriber immediately.
Pancreatitis
Acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing cases, has been observed with GLP-1 receptor agonists including liraglutide. The Saxenda prescribing information states that patients should be monitored for signs and symptoms of pancreatitis after initiating or increasing the dose. If pancreatitis is suspected — sudden, severe abdominal pain that may radiate to the back, with or without vomiting — patients should stop liraglutide immediately and seek emergency care. Do not restart without a formal physician re-evaluation. Liraglutide has not been studied in patients with prior pancreatitis, and the prescribing information advises against its use in that population.
Hypoglycemia With Insulin or Sulfonylureas
Liraglutide alone carries low intrinsic hypoglycemia risk because insulin stimulation is glucose-dependent and turns down as blood sugar normalizes. That changes when liraglutide is combined with insulin or a sulfonylurea (for example, glipizide or glyburide). The FDA labeling warns that adults with type 2 diabetes on an insulin secretagogue or insulin face increased hypoglycemia risk when Saxenda is added; dose reductions of the concomitant agent are typically required.
Other Notable Warnings
Heart rate: Clinical monitoring in SCALE trials found mean resting heart rate increases of 2 to 3 beats per minute with liraglutide versus placebo. The prescribing information recommends monitoring at regular intervals and discontinuing liraglutide if a sustained, clinically significant resting heart rate elevation is observed.
Gallbladder disease: Cholelithiasis occurred in 2.2% of Saxenda-treated patients versus 0.8% in the placebo arm in clinical trials. Right upper quadrant pain or other gallbladder symptoms warrant workup.
Pregnancy: Liraglutide should be discontinued when pregnancy is recognized. Weight loss during pregnancy offers no benefit and may cause fetal harm; animal studies showed embryonic deaths and fetal abnormalities at exposures approximating clinical levels. Women planning pregnancy should discuss discontinuation timing with their physician in advance.
Compounded liraglutide: The FDA has explicitly cautioned that compounded liraglutide products are not FDA-approved and have not been evaluated for safety, purity, or potency. Any product claiming to contain liraglutide that is not the approved Victoza or Saxenda pen falls outside the manufacturing safeguards and regulatory oversight that backed the SCALE and LEADER trials.
Daily vs. Weekly: Where Liraglutide Fits Now
The practical question most patients and clinicians face: given that once-weekly semaglutide and tirzepatide now exist, why choose a once-daily drug? A few reasons remain clinically sound.
Titration granularity. Liraglutide's five-step escalation — 0.6 mg, 1.2 mg, 1.8 mg, 2.4 mg, 3 mg — lets a prescriber hold at an intermediate dose if gastrointestinal tolerance is limiting. A missed daily injection carries a shorter pharmacological shadow than a missed weekly dose.
Pediatric-specific approval. Saxenda remains the only GLP-1 weight-management agent with dedicated FDA approval in adolescents aged 12 and older, based on actual pediatric trial data rather than adult extrapolation. For prescribers and payers, that label distinction matters.
Efficacy trade-off. Liraglutide produces roughly 5 to 6 kg more weight loss than placebo over 56 weeks. Semaglutide 2.4 mg (Wegovy) produces approximately 12 kg more than placebo over 68 weeks, and tirzepatide reaches 20 to 21 percent mean body weight reduction. Patients not reaching meaningful response thresholds after adequate titration on liraglutide have a clear, evidence-based pathway to a more efficacious agent. Those who do respond adequately have no pharmacological imperative to switch.
Liraglutide is not an outdated molecule — it is a well-characterized drug with 15 years of post-market history. It is, however, a less efficacious weight-loss agent than what followed it, and daily injection represents a genuine adherence burden for some patients.
For more on how the different GLP-1 agents compare in terms of weight outcomes and mechanism, see semaglutide: complete guide and peptides for weight loss.
Frequently Asked Questions
Is liraglutide available as a generic?
No. As of 2026, neither Victoza nor Saxenda has a generic equivalent approved in the United States. Both remain branded Novo Nordisk products, which carries direct cost implications.
Can Victoza be used for weight loss, or Saxenda for diabetes?
No, not per FDA-approved labeling. The doses differ — Victoza tops at 1.8 mg, Saxenda at 3 mg — and the trial evidence for each indication was generated at the dose on each brand's label. Using either product outside its approved indication is off-label.
What happens to weight after stopping Saxenda?
Evidence from the GLP-1 class broadly shows weight loss is not sustained after stopping the medication. The mechanisms — reduced appetite signaling, slowed gastric emptying — are active only during treatment. Patients should discuss the long-term management plan with their prescriber before initiating.
Can liraglutide be used alongside other GLP-1 agonists?
No. The Saxenda prescribing information explicitly states it is not recommended in combination with other liraglutide-containing products or other GLP-1 receptor agonists. Combining two agents in the same class provides no established benefit and increases adverse-effect risk.
Conclusion
Liraglutide (Victoza, Saxenda) is the foundational daily GLP-1 receptor agonist — the molecule that established proof of concept for this class in both type 2 diabetes and weight management before once-weekly options existed. The SCALE trials showed real, statistically significant weight loss. The LEADER trial demonstrated a cardiovascular mortality benefit in high-risk T2D that remains clinically meaningful. The pediatric Saxenda approval covers an age group for which dedicated trial evidence and regulatory clarity still distinguish it from newer weekly agents.
The actionable takeaway: liraglutide is a prescription drug requiring physician oversight, carries an absolute contraindication in MEN-2 and personal or family history of MTC, and poses a pancreatitis risk demanding immediate emergency care if symptoms arise. For most patients beginning weight management pharmacotherapy today, a prescriber will likely lead with a weekly agent — but for patients who tolerate daily dosing, require the pediatric label, or who achieved adequate response and have no reason to switch, liraglutide remains a clinically sound, evidence-backed choice.
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Liraglutide (Victoza, Saxenda) is a prescription drug regulated by the FDA; it is not available without a valid prescription from a licensed healthcare provider. The safety warnings described in this article — including the boxed warning for thyroid C-cell tumors, pancreatitis risk, and hypoglycemia risk with concomitant insulin or sulfonylureas — are not exhaustive. Always read the full FDA-approved prescribing information, consult a licensed physician or pharmacist before starting, changing, or stopping any prescription medication, and seek emergency medical care immediately if you experience sudden severe abdominal pain or any other symptom that may indicate a serious adverse event.
