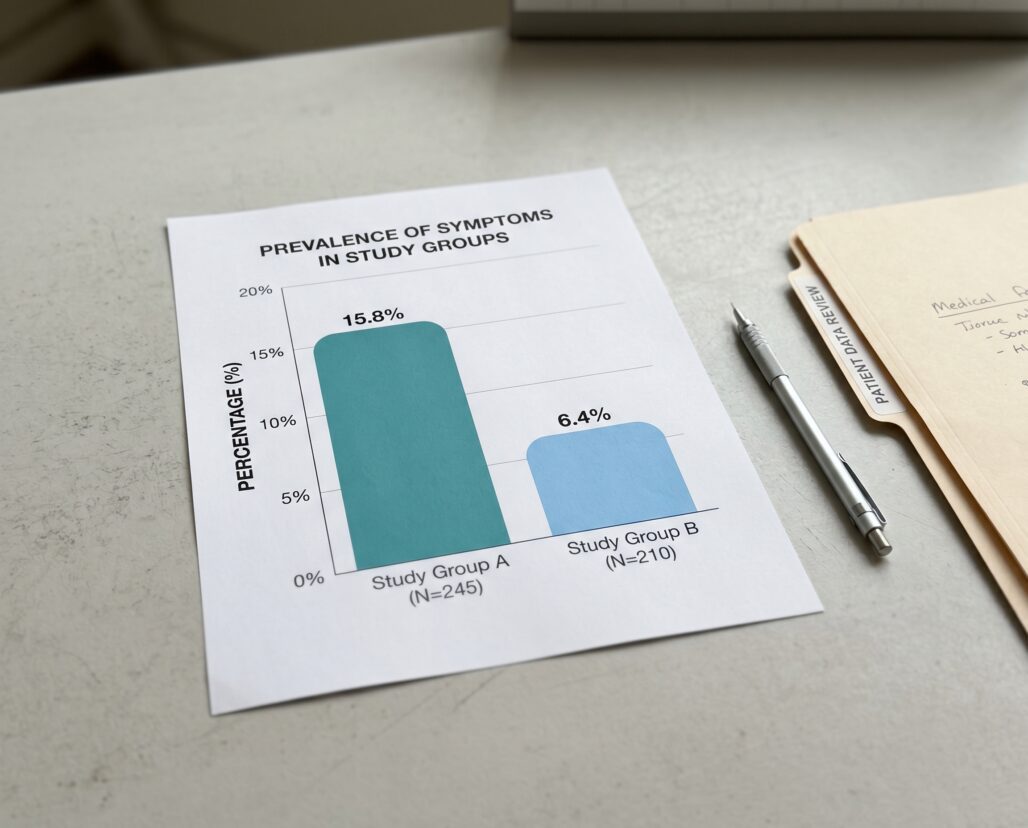
You have probably heard the names Ozempic and Saxenda in the same breath at some point, as if they are interchangeable. They are not. Both belong to the same drug class, both reduce body weight, and both are injectable. But one is dosed once a week, the other every single day, and the head-to-head clinical evidence shows a weight-loss difference so large that calling the two drugs equivalent would misrepresent the data. If you are trying to understand whether semaglutide or liraglutide is the stronger choice for weight management, the honest summary is: the STEP 8 trial found that weekly semaglutide 2.4 mg produced 15.8% body weight loss versus 6.4% with daily liraglutide 3 mg over 68 weeks, while discontinuation rates nearly doubled on the daily drug.
That said, efficacy numbers from a clinical trial do not decide which medication a specific patient should use. Prescriber judgment, insurance coverage, comorbidities, and tolerability all matter. This article walks through the clinical evidence and the practical trade-offs so you can have a more informed conversation with your prescriber.
Summary: Same Class, Different Profiles
Semaglutide and liraglutide are both glucagon-like peptide-1 (GLP-1) receptor agonists — peptide-based drugs that mimic the gut hormone GLP-1 to reduce appetite, slow gastric emptying, and promote satiety. They share a mechanism at the receptor level, a similar side-effect signature dominated by gastrointestinal symptoms, and an identical boxed warning about thyroid C-cell tumors in rodent studies.
Where they diverge is in molecular structure, half-life, and — critically — the weight-loss magnitude supported by clinical trials. Semaglutide has a much longer half-life, allowing once-weekly dosing. Liraglutide's shorter half-life requires daily injection. The structural difference is not trivial: it produces a measurable difference in sustained receptor engagement that the head-to-head evidence suggests translates into meaningfully greater weight loss.
For an in-depth look at semaglutide's pharmacology and the full STEP trial program, see the semaglutide complete guide. For liraglutide's mechanism and the SCALE trial data, see the liraglutide Saxenda and Victoza explainer.
Brand Names Clarified: What Drug Is in Which Pen
The brand landscape for both drugs is a genuine source of confusion, and it matters for understanding which approvals apply to weight management.
Semaglutide comes in three brands. Ozempic (0.5-2 mg weekly, subcutaneous) and Rybelsus (7-14 mg oral daily) are approved for T2D. Wegovy (2.4 mg weekly, subcutaneous) is approved for chronic weight management. When research and clinical discussions concern obesity treatment, they mean the Wegovy dose — not Ozempic, even though the molecule is identical.
Liraglutide comes in two brands. Victoza (1.2-1.8 mg daily) is approved for T2D. Saxenda (3.0 mg daily) is approved for chronic weight management under the same BMI criteria as Wegovy. STEP 8 and the SCALE weight-management trials specifically used these higher approved doses.
If someone says they are "using Ozempic to lose weight," that is an off-label application of a diabetes drug, not the weight-management-labeled formulation.
Mechanism: How Similar Is Similar Enough?
Both drugs bind and activate the GLP-1 receptor, a G protein-coupled receptor expressed in the pancreas, hypothalamus, gut, and other tissues. The shared mechanism produces overlapping effects: reduced appetite signaling in the brain, slower gastric emptying that prolongs the sensation of fullness, and stimulation of glucose-dependent insulin secretion from beta cells.
The structural difference lies in degradation resistance. Liraglutide attaches a fatty acid chain that allows albumin binding, extending its half-life to roughly 13 hours and requiring daily dosing. Semaglutide adds a larger fatty acid linker plus amino acid substitutions that resist enzymatic breakdown, producing a half-life of approximately one week and enabling once-weekly dosing. The sustained receptor engagement achieved with semaglutide is one proposed explanation for its greater efficacy, though the precise mechanism remains under investigation.
STEP 8: The Head-to-Head That Settled the Comparison
Until STEP 8, the two drugs had only been compared indirectly through separate placebo-controlled trials. The STEP 8 randomized clinical trial (NCT04074161) changed that by putting both drugs in the same study with the same population and the same design.
Published in JAMA in January 2022 (Rubino et al., JAMA 2022;327(2):138-150, PMID 35015037), the trial enrolled 338 adults with a BMI of 30 or above, or 27 with comorbidities, without diabetes. The mean age was 49 years and 78.4% of participants were female. Participants were randomized to once-weekly subcutaneous semaglutide 2.4 mg (n=126), once-daily subcutaneous liraglutide 3.0 mg (n=127), or pooled placebo (n=85), over 68 weeks. Both active groups received diet and physical activity counseling alongside the drug.
The primary outcome was percentage change in body weight from baseline. Semaglutide participants lost a mean of 15.8% of body weight. Liraglutide participants lost 6.4%. The between-group difference of 9.4 percentage points was statistically significant at p less than 0.001. This is not a marginal difference. In a drug class where a 5% weight loss is considered clinically meaningful, a 9.4-point gap between two drugs in the same class is a large effect.
The secondary responder thresholds make the separation even clearer. Among those on semaglutide, 70.9% achieved at least 10% body weight loss compared with 25.6% on liraglutide (odds ratio 6.3). For 15% or greater loss, the figures were 55.6% versus 12.0% (OR 7.9). For 20% or greater, 38.5% versus 6.0% (OR 8.2). In practical terms, more than one in three participants on semaglutide lost at least a fifth of their body weight. Fewer than one in fourteen on liraglutide reached that threshold.
The gastrointestinal side-effect rates were comparable: 84.1% on semaglutide and 82.7% on liraglutide experienced at least one GI event. The meaningful difference emerged in who stayed on treatment. Discontinuation rates were 13.5% for semaglutide and 27.6% for liraglutide. The daily injection burden may have contributed to that gap, but the study design does not allow a definitive causal claim.
For reference: the SCALE Obesity and Prediabetes trial (Pi-Sunyer et al., NEJM 2015, PMID 26132939) found liraglutide 3.0 mg produced 8.4 kg mean weight loss versus 2.8 kg for placebo over 56 weeks, with 63.2% achieving at least 5% loss. The STEP 1 placebo-controlled trial for semaglutide 2.4 mg found roughly 15% mean weight loss over 68 weeks. These single-arm-versus-placebo results cannot substitute for a direct comparison, but they bracket the efficacy pattern STEP 8 confirmed head-to-head.
Side Effects Compared
The side-effect profiles of semaglutide and liraglutide overlap substantially because they share the same receptor mechanism.
Gastrointestinal events are the dominant tolerability concern for both. Nausea, vomiting, diarrhea, and constipation are common during dose escalation and typically decrease over time. Both drugs use a gradual titration schedule to mitigate these effects, and GI events account for a significant share of discontinuations in both groups.
Pancreatitis is a serious risk listed in the prescribing information for both drugs. Patients should discontinue the medication if pancreatitis is suspected and not restart it if acute pancreatitis is confirmed. Any persistent severe abdominal pain, especially pain radiating to the back, should prompt immediate medical evaluation.
Hypoglycemia is a risk primarily when either drug is combined with sulfonylureas or insulin. In non-diabetic patients on either drug alone, clinically significant hypoglycemia is uncommon because GLP-1-stimulated insulin release is glucose-dependent. Patients on multi-drug regimens should discuss dose adjustments before adding either GLP-1 agonist.
Heart rate increase is a pharmacological effect of both drugs. Clinical significance depends on baseline cardiovascular status and should be discussed with the prescribing provider.
Gallbladder disease, including cholelithiasis and cholecystitis, appears at higher rates with both drugs compared to placebo. Rapid weight loss itself increases gallstone risk, which confounds attribution to the drug.
Thyroid C-cell tumors carry a boxed warning for both semaglutide and liraglutide. In rodent studies at clinically relevant exposures, both drugs caused thyroid C-cell tumors, including medullary thyroid carcinoma. The human relevance of this finding is uncertain, but both drugs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). This warning applies equally to both drugs and is not a distinction between them.
The tolerability difference seen in STEP 8 — roughly double the discontinuation rate on liraglutide — is not explained by a difference in the type of side effects, since both caused GI events at similar rates. The leading hypothesis is that daily injection simply imposes a higher daily burden on patients, making dropout more likely when tolerability problems arise.
Daily vs. Weekly: The Dosing Cadence Trade-Off
The dosing frequency difference between these two drugs is not a convenience detail. It has practical implications for adherence, lifestyle fit, and consistent drug exposure.
Semaglutide 2.4 mg (Wegovy) is injected once per week on the same day each week, regardless of meals. The starting dose is 0.25 mg, titrated over 16 weeks to the 2.4 mg maintenance dose. A missed weekly dose is recoverable within two days without restarting titration, and the long half-life means plasma levels do not drop sharply from a single missed injection.
Liraglutide 3.0 mg (Saxenda) is injected once daily at approximately the same time each day. The starting dose of 0.6 mg titrates weekly in 0.6 mg increments to 3.0 mg over four weeks — a faster ramp-up than semaglutide. Because the 13-hour half-life produces meaningful day-to-day concentration swings, consistent daily adherence matters more than it does with the weekly drug.
For patients who find daily injection burdensome, semaglutide's weekly schedule is a clear practical advantage. The STEP 8 discontinuation data — 13.5% vs 27.6% — suggest this burden translates into real-world dropout, though the study design does not allow a definitive causal attribution to dosing frequency alone.
Cost and Access
Drug pricing is highly dynamic and varies by insurance plan, pharmacy benefit structure, pharmacy location, and patient assistance program eligibility. General patterns as of 2025 are as follows.
Wegovy (semaglutide 2.4 mg) carries a list price in the United States of approximately $1,350 to $1,500 per month for the maintenance dose. Saxenda (liraglutide 3.0 mg) lists at approximately $1,300 to $1,400 per month. The difference in list price is modest. The difference in practical out-of-pocket cost is driven almost entirely by insurance formulary decisions, and those vary enormously by plan.
Neither drug is a generic. Liraglutide was approved earlier (Saxenda received FDA approval in December 2014 under NDA 206321), and semaglutide for weight management came later (Wegovy received FDA approval in June 2021 under NDA 215256). The older approval for liraglutide does not translate to a price advantage at present.
One important caveat: the FDA has issued explicit safety cautions about compounded semaglutide products made during periods of Wegovy shortage. Compounded drugs are not FDA-approved, have not been verified for potency or sterility to the same standards as the commercial product, and have been associated with reported adverse events. Patients should discuss the source and regulatory status of any compounded formulation with their prescriber before using it. Novo Nordisk manufactures both Wegovy and Saxenda and offers patient assistance programs worth exploring for income-qualified patients.
Side-by-Side Table
| Property | Semaglutide (Wegovy) | Liraglutide (Saxenda) |
|---|---|---|
| Drug class | GLP-1 receptor agonist | GLP-1 receptor agonist |
| Weight management brand | Wegovy | Saxenda |
| T2D brand | Ozempic, Rybelsus | Victoza |
| Dosing frequency | Once weekly (subcutaneous) | Once daily (subcutaneous) |
| Maintenance dose | 2.4 mg/week | 3.0 mg/day |
| Half-life | ~7 days | ~13 hours |
| FDA approval (weight) | June 2021 (NDA 215256) | December 2014 (NDA 206321) |
| Mean weight loss (STEP 8) | 15.8% at 68 weeks | 6.4% at 68 weeks |
| Discontinuation rate (STEP 8) | 13.5% | 27.6% |
| Thyroid C-cell boxed warning | Yes (both drugs) | Yes (both drugs) |
| Pancreatitis warning | Yes (both drugs) | Yes (both drugs) |
| Contraindicated in MEN 2 | Yes | Yes |
| Pregnancy | Discontinue | Discontinue |
| Approximate monthly list price | $1,350-$1,500 | $1,300-$1,400 |

FAQ
Is Ozempic the same as Wegovy?
No. Both contain semaglutide, but Ozempic is dosed at up to 2 mg weekly and is approved for type 2 diabetes. Wegovy is dosed at 2.4 mg weekly and is approved specifically for chronic weight management. Using Ozempic for weight loss without a T2D diagnosis is an off-label application.
Is Saxenda the same as Victoza?
No. Both contain liraglutide, but Victoza is dosed at up to 1.8 mg daily for type 2 diabetes, and Saxenda is dosed at 3.0 mg daily for weight management. The drugs differ in their approved doses and indications.
Can I switch from liraglutide to semaglutide?
That is a question for your prescriber. Switching is mechanistically feasible, but timing and dose overlap require individualized clinical guidance.
What if I cannot afford Wegovy or Saxenda?
Manufacturer assistance programs and insurance formulary appeals are the first steps. A prescriber or pharmacist can identify eligibility. Some plans cover one drug but not the other, so a formulary check before the prescription is written saves time.
What about the thyroid cancer risk?
The boxed warning is based on rodent studies and applies to both drugs. Human relevance has not been established, but neither drug should be used in patients with personal or family history of medullary thyroid carcinoma or MEN 2 syndrome. Routine calcitonin monitoring is not recommended in the absence of symptoms or family history.
Is semaglutide always better than liraglutide?
The STEP 8 head-to-head trial showed a large efficacy advantage for semaglutide at the approved weight-management doses. For patients who cannot tolerate semaglutide, who have specific insurance constraints, or for whom a prescriber has clinical reasons to prefer liraglutide, the older drug retains meaningful evidence of benefit. Nearly one in three liraglutide patients achieved more than 10% weight loss in STEP 8, which is a clinically significant outcome.
Conclusion: What the Evidence Actually Supports
The clinical picture from STEP 8 is cleaner than head-to-head evidence often is in pharmacology. Semaglutide 2.4 mg once weekly produced weight loss that was more than twice that of liraglutide 3.0 mg once daily in the same trial, in the same population, over the same duration. The 9.4-percentage-point difference in mean body weight reduction, the two- to eightfold differences in responder rates across thresholds, and the near-halving of discontinuation rates all point in the same direction.
For patients considering GLP-1 receptor agonists for weight management and curious how this class compares with newer entrants, a review of the Ozempic vs. Mounjaro comparison covers tirzepatide, which adds a GIP receptor mechanism to the picture.
Actionable takeaways from the evidence:
- If your prescriber is choosing between the two for weight management, ask specifically about the STEP 8 data and your own candidacy for each drug.
- If you are already on daily liraglutide and have not reached target weight, discuss the STEP 8 results with your prescriber, since the data support a meaningful efficacy difference.
- If cost or insurance coverage limits access to Wegovy, patient assistance programs from the manufacturer are worth exploring before accepting that coverage is unavailable.
- Avoid compounded semaglutide products unless your prescriber has specifically evaluated the source — the FDA has flagged safety concerns with compounded formulations.
Both drugs carry the same thyroid C-cell tumor boxed warning, the same pancreatitis caution, and the same instruction to discontinue during pregnancy. Neither is appropriate for self-directed use without medical supervision. The efficacy difference shown in STEP 8 does not change those baseline safety considerations.
The information in this article is educational and is not a substitute for professional medical advice, diagnosis, or treatment. GLP-1 receptor agonists including semaglutide and liraglutide are prescription medications. Speak with a licensed healthcare provider before starting, stopping, or adjusting any medication. Individual responses to these drugs vary, and the clinical trial results described here represent group averages, not guaranteed individual outcomes.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
