If you are reading about Trulicity because someone in your life takes it for weight loss, the first thing worth knowing is that dulaglutide does not have an FDA-approved weight-management indication. It never has. The confusion is understandable — Trulicity belongs to the same GLP-1 receptor agonist drug class as Ozempic and Wegovy, and the class has become inseparable from obesity coverage in the media. Dulaglutide was approved in 2014 for glycemic control in type 2 diabetes, and that label has not changed. What makes it worth understanding on its own terms is the REWIND cardiovascular outcomes trial — 9,901 patients, 5.4-year median follow-up, and a statistically significant MACE reduction that extended to people who had never had a heart attack or stroke. The bottom line: dulaglutide is a once-weekly GLP-1 injection for type 2 diabetes with a meaningful cardiovascular outcomes story and no approved role in weight management.
Summary
Dulaglutide (Trulicity, Eli Lilly) is a GLP-1 receptor agonist approved by the FDA in September 2014 for adults and pediatric patients aged 10 and older with type 2 diabetes. It is also approved to reduce the risk of major adverse cardiovascular events in adults with T2D who have established cardiovascular disease or multiple cardiovascular risk factors. It is not FDA-approved for weight management.
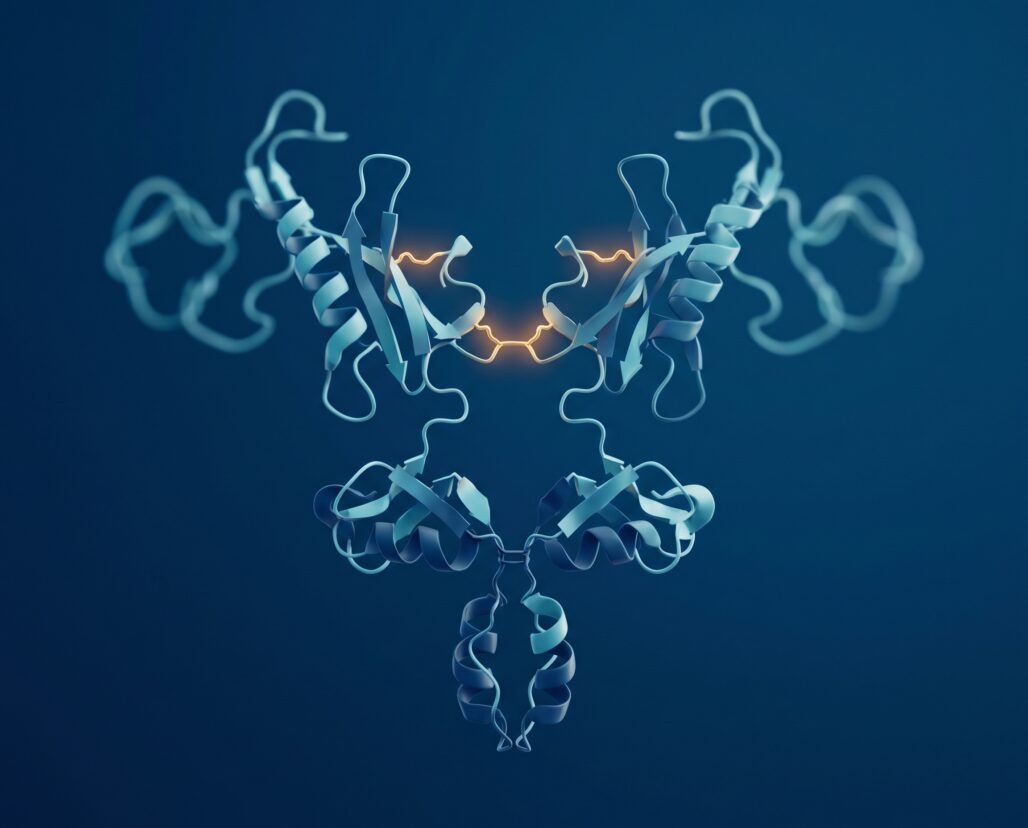
- Mechanism: A fusion protein consisting of two GLP-1 analog chains linked by disulfide bonds and attached to a modified IgG4 Fc domain, giving it a half-life of approximately five days and enabling once-weekly dosing.
- Dosing: Starts at 0.75 mg once weekly via single-dose auto-injector; can be titrated up to 1.5 mg, 3 mg, or 4.5 mg every four weeks as needed for glycemic goals.
- T2D efficacy: The AWARD phase 3 program (11 trials) showed HbA1c reductions of approximately 0.7 to 1.6 percentage points versus active comparators including exenatide, sitagliptin, insulin glargine, liraglutide, and metformin, with 1.5 mg consistently superior to comparators in most arms (PMID 27102969).
- CV outcomes: REWIND trial (n=9,901, median 5.4 years) showed a hazard ratio of 0.88 (95% CI 0.79-0.99, p=0.026) for the primary MACE composite versus placebo (PMID 31189511).
- Pediatric approval: AWARD-PEDS confirmed efficacy in youth aged 10 to 17 with T2D, with HbA1c reductions of 0.6 to 0.9 percentage points versus placebo worsening by 0.6 points (PMID 35658022).
- Boxed warning: Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN-2) is an absolute contraindication. Thyroid C-cell tumor risk in humans is unknown.
- Not a weight drug: No Trulicity equivalent of Wegovy or Saxenda exists. Dulaglutide causes modest weight loss or weight-gain attenuation as a secondary effect but is not approved for, nor indicated in, chronic weight management.
What Dulaglutide Is: The GLP-1 Plus IgG4 Fc Architecture
Most GLP-1 receptor agonists achieve extended half-life through albumin binding, acylation, or polyethylene glycol attachment. Dulaglutide uses a different structural strategy. According to the Trulicity prescribing information, the molecule is "a fusion protein that consists of 2 identical, disulfide-linked chains, each containing a modified GLP-1 analog sequence covalently linked to the Fc portion of a modified human immunoglobulin G4 (IgG4) heavy chain." Think of it as a peptide stapled to an antibody scaffold: the Fc domain gives the molecule antibody-like stability and a half-life long enough to permit subcutaneous injection just once a week. The IgG4 modification reduces Fc receptor binding to minimize immune activation.
This Fc-fusion architecture produces a 59-kilodalton molecule with a mean half-life of approximately five days, enabling dulaglutide to occupy GLP-1 receptors on pancreatic beta cells, alpha cells, and neurons in a sustained, low-fluctuation manner across the dosing interval.
GLP-1 receptors on beta cells amplify insulin secretion in a glucose-dependent fashion, meaning insulin release tracks rising blood glucose rather than firing continuously — unlike sulfonylureas, which force insulin release regardless of glucose levels. On alpha cells, GLP-1 receptor activation suppresses glucagon, reducing fasting hepatic glucose output. In the brain and gut, GLP-1 receptor signaling reduces appetite and slows gastric emptying, producing the nausea that is a class-wide side effect and the modest secondary weight-loss effect that is real but not approved.
For a broader explanation of how GLP-1 receptor agonists fit within the peptide drug category, see the FDA-approved peptides overview and what are peptides.
The AWARD Trial Program: T2D Efficacy Across 11 Studies
Eli Lilly built the regulatory case for dulaglutide through the AWARD (Assessment of Weekly Administration of LY2189265 in Diabetes) phase 3 program, ultimately spanning 11 trials across multiple T2D populations and backgrounds. The review published in Diabetes, Metabolism Research and Reviews (PMID 27102969) summarized the first six completed trials and found that the 1.5 mg dose was superior to active comparators in five of those six studies on the primary HbA1c endpoint. The 0.75 mg dose was superior in four of five applicable trials and non-inferior to insulin glargine in AWARD-2.
Comparators across the AWARD program included exenatide twice daily, sitagliptin, metformin, insulin glargine (two separate trials), and liraglutide once daily. Beating a DPP-4 inhibitor or exenatide is a relatively accessible bar in this class. The more meaningful comparisons were against insulin glargine, where dulaglutide held its ground without the hypoglycemia burden and without requiring blood glucose monitoring for most patients. The liraglutide comparison in AWARD-6 was designed as a non-inferiority test; dulaglutide 1.5 mg showed non-inferiority and in one secondary analysis numerically superior HbA1c reduction.
Later AWARD trials extended the evidence base to patients on SGLT2 inhibitors (AWARD-10, PMID 29483060), patients with moderate-to-severe chronic kidney disease (AWARD-7, PMID 29910024), and higher-dose arms at 3 mg and 4.5 mg (AWARD-11, PMID 33397768), which confirmed incremental HbA1c and weight reductions and explain why the label now lists four strengths. A skeptical read: dulaglutide's comparative weight-loss effects are modest relative to semaglutide, and the absence of a dedicated obesity trial means it never built the evidence base for a weight-management indication — a regulatory gap, not necessarily a pharmacological ceiling.
REWIND: The Cardiovascular Outcomes Trial
The REWIND trial (Researching Cardiovascular Events with a Weekly Incretin in Diabetes) reported in The Lancet in 2019 (PMID 31189511, Gerstein et al.) and represents the most clinically distinctive data point in the dulaglutide story. The trial randomized 9,901 participants with type 2 diabetes to 1.5 mg dulaglutide or placebo at 371 sites across 24 countries, following them for a median of 5.4 years.
Two features made REWIND methodologically unusual compared to other GLP-1 cardiovascular outcomes trials. First, the baseline HbA1c was lower than most comparable trials — median 7.2% — meaning the population was more representative of well-managed T2D patients than of those with poor glycemic control requiring intensification. Second, roughly 31% of participants had no established cardiovascular disease at baseline; they were enrolled on the basis of cardiovascular risk factors alone. Most CVOT trials for this class required prior cardiovascular events.
The primary endpoint was a composite of non-fatal myocardial infarction, non-fatal stroke, or cardiovascular death (three-point MACE). The result: 12.0% incidence in the dulaglutide group versus 13.4% with placebo, producing a hazard ratio of 0.88 (95% CI 0.79-0.99, p=0.026). That is a 12% relative risk reduction that crossed the pre-specified superiority threshold.
Secondary endpoints showed a reduction in new or worsening diabetic kidney disease (HR 0.85, 95% CI 0.77-0.93), though all-cause mortality did not reach statistical significance (HR 0.90, p=0.067). Gastrointestinal adverse events occurred in 47.4% of dulaglutide-treated participants versus 34.1% in the placebo group.
One honest qualification: a 12% relative risk reduction on a 13% baseline event rate translates to approximately 1.4 percentage points of absolute risk reduction over 5.4 years. That is meaningful but modest. Semaglutide (Ozempic) carries a comparable CV indication and showed a 20% MACE reduction in SELECT — a relevant benchmark for class-level prescribing decisions.
Side Effects and the Boxed Warning
The most common adverse reactions with dulaglutide are gastrointestinal: nausea, diarrhea, vomiting, abdominal pain, and decreased appetite. These occur in 32-41% of patients depending on dose and are most pronounced during dose initiation and escalation, typically improving over the first four to eight weeks. They are a class effect of GLP-1 receptor agonists and are mechanistically linked to slowed gastric emptying.
The prescribing information carries a boxed warning about thyroid C-cell tumors, the same warning that applies to all GLP-1 receptor agonists. Dulaglutide caused dose-dependent thyroid C-cell tumors in rats; whether this translates to humans is unknown. What is not unknown is the contraindication: dulaglutide must not be used in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN-2). Prescribers are instructed to counsel patients to report any neck masses, dysphagia, difficulty breathing, or persistent hoarseness.
Acute pancreatitis — including fatal and non-fatal hemorrhagic and necrotizing forms — has been observed with GLP-1 receptor agonists including dulaglutide. Patients should be told to seek immediate care if they experience severe, persistent abdominal pain that radiates to the back. Dulaglutide should be discontinued if pancreatitis is confirmed and not restarted.
Hypoglycemia risk is low when dulaglutide is used as monotherapy or with metformin. However, when combined with insulin secretagogues such as sulfonylureas or with insulin itself, hypoglycemia risk rises significantly. The prescribing information recommends reducing the dose of the concomitant agent.
Regarding pregnancy: the label advises discontinuing dulaglutide well before a planned pregnancy; at minimum, the drug should be stopped when pregnancy is confirmed. Animal studies showed fetal abnormalities at exposures above human therapeutic levels. The FDA pregnancy category for dulaglutide is listed as "use only if the potential benefit justifies the potential risk to the fetus."
A note on compounded dulaglutide: unlike semaglutide, which became widely available through compounding pharmacies during the Ozempic shortage period, compounded dulaglutide has not generated the same scale of market. However, the FDA's general position on compounded versions of FDA-approved GLP-1 drugs is explicit — compounded formulations are not FDA-approved, have not been demonstrated safe or effective, and may not be equivalent to the approved product. Patients should use only the brand-name, pharmacy-dispensed Trulicity prescribed by a licensed clinician.
Dosing and the Single-Dose Auto-Injector
Trulicity is supplied as a single-dose auto-injector pen in four strengths: 0.75 mg/0.5 mL, 1.5 mg/0.5 mL, 3 mg/0.5 mL, and 4.5 mg/0.5 mL. The starting dose for most patients is 0.75 mg once weekly. If additional glycemic control is needed, the dose can be increased in 0.75 mg increments every four weeks, up to the maximum of 4.5 mg once weekly.
The auto-injector hides the needle before, during, and after injection. Patients press the device against the skin — abdomen, thigh, or upper arm — push a button, and hold for about five seconds. No mixing or reconstitution is required. Dose timing is flexible: any day of the week, with or without food. If a dose is missed and the next scheduled dose is more than three days away, take the missed dose immediately. If fewer than three days remain, skip it and resume the regular schedule — never double-dose in a single week.
Where Dulaglutide Sits Versus Ozempic and Mounjaro
The once-weekly GLP-1 market now includes semaglutide (Ozempic) and tirzepatide (Mounjaro, a dual GIP/GLP-1 agonist). On head-to-head HbA1c reduction, SUSTAIN-7 showed semaglutide 1 mg outperforms dulaglutide 1.5 mg on both glucose and weight. Tirzepatide's SURPASS program showed even larger effects. If maximizing HbA1c reduction or weight loss is the treatment priority, dulaglutide is not the first choice by the numbers.
Where dulaglutide can be a reasonable choice: patients with insurance formulary constraints that favor Trulicity, those who prefer the single-dose auto-injector format, and — critically — patients with multiple CV risk factors but no established CVD event. REWIND specifically enrolled this secondary-prevention population, and the risk-reduction data there is the drug's most distinctive clinical asset. REWIND's 12% relative MACE reduction is smaller than semaglutide's numbers in SELECT, but it is the only trial in this class powered to show superiority in a mixed primary-and-secondary prevention population. Dulaglutide is not the class leader on any single efficacy dimension, but it is a well-studied drug with a decade of safety data and a CV outcomes story that holds up to scrutiny.
For a detailed comparison, see Ozempic vs Trulicity and the semaglutide complete guide.

Frequently Asked Questions
Is Trulicity approved for weight loss? No. Dulaglutide does not have an FDA weight-management indication. It causes modest secondary weight reduction — approximately one to three kilograms in clinical trials — but this is not its approved purpose. There is no Trulicity equivalent of Wegovy or Saxenda. Prescribing it off-label for weight loss is a clinician's prerogative, but it is not supported by large dedicated obesity trials.
Can dulaglutide be used in patients with kidney disease? AWARD-7 (PMID 29910024) showed dulaglutide was effective in moderate-to-severe CKD with slower eGFR decline versus insulin glargine. No renal dose adjustment is required, but clinical judgment applies; consult a nephrologist at CKD stage 4 or 5.
How does dulaglutide interact with insulin? Combination use increases hypoglycemia risk. The prescribing information recommends reducing insulin or sulfonylurea dose when adding dulaglutide, and counseling patients on hypoglycemia recognition.
Can children take Trulicity? Yes. The AWARD-PEDS trial (PMID 35658022) confirmed efficacy and a consistent safety profile in youth aged 10 to 17 with type 2 diabetes, and the FDA label covers pediatric patients from age 10 onward.
What happens if I miss a dose? If the next weekly injection is more than three days away, take the missed dose as soon as you remember. If the next dose is within three days, skip the missed dose and resume the regular schedule. Do not take two doses in one week.
The Bottom Line on Dulaglutide
Dulaglutide is a well-characterized GLP-1 receptor agonist for type 2 diabetes with a decade of real-world clinical use. Its Fc-fusion architecture achieves once-weekly dosing, its AWARD trial program established efficacy across a broad range of T2D populations, and REWIND adds a meaningful CV outcomes signal that extends specifically to patients without prior cardiovascular events — the population where comparable data from other GLP-1 agents is thinnest.
It is not the most potent agent in the class on glycemic reduction. It carries the boxed warning about thyroid C-cell tumors, a serious pancreatitis risk, and no approved weight-management indication. Compounded dulaglutide falls outside FDA oversight and should be avoided.
For patients with T2D and multiple cardiovascular risk factors who have not yet had a cardiac event, dulaglutide's REWIND data is a clinically distinctive asset. For patients where weight loss is the primary goal, a clinician should assess whether a GLP-1 agent with a dedicated obesity indication is more appropriate.
Next steps: If you are trying to understand how dulaglutide compares to the broader GLP-1 class, the semaglutide complete guide covers the SUSTAIN and STEP trial programs in detail, and the Ozempic vs Trulicity comparison addresses the head-to-head clinical data directly. Neither article substitutes for a conversation with a physician who knows your metabolic history.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
