Peptide marketing runs on two speeds: "feel it tomorrow" and "results in 30 days." Both are fiction for most of what people actually buy. The honest answer to how long peptides take to work depends almost entirely on which molecule you mean, which outcome you are measuring, and whether your compound is FDA-approved with controlled trial data behind it or a grey-market research chemical that has never been tested in humans under controlled conditions. Conflating them is how people set unrealistic expectations, abandon effective treatments too early, and stay on ineffective ones too long. This article gives you the evidence-backed timelines that exist and is explicit about where no reliable human timeline data exists at all.
For background on what peptides are biologically, see what are peptides. For a full safety profile, read are peptides safe.
Summary
Peptide onset ranges from 45 minutes (bremelanotide) to 8 weeks (detectable collagen skin changes) to 52 weeks (GLP-1 weight-loss plateau). For grey-market peptides, honest answer: no human RCT timeline data exists.
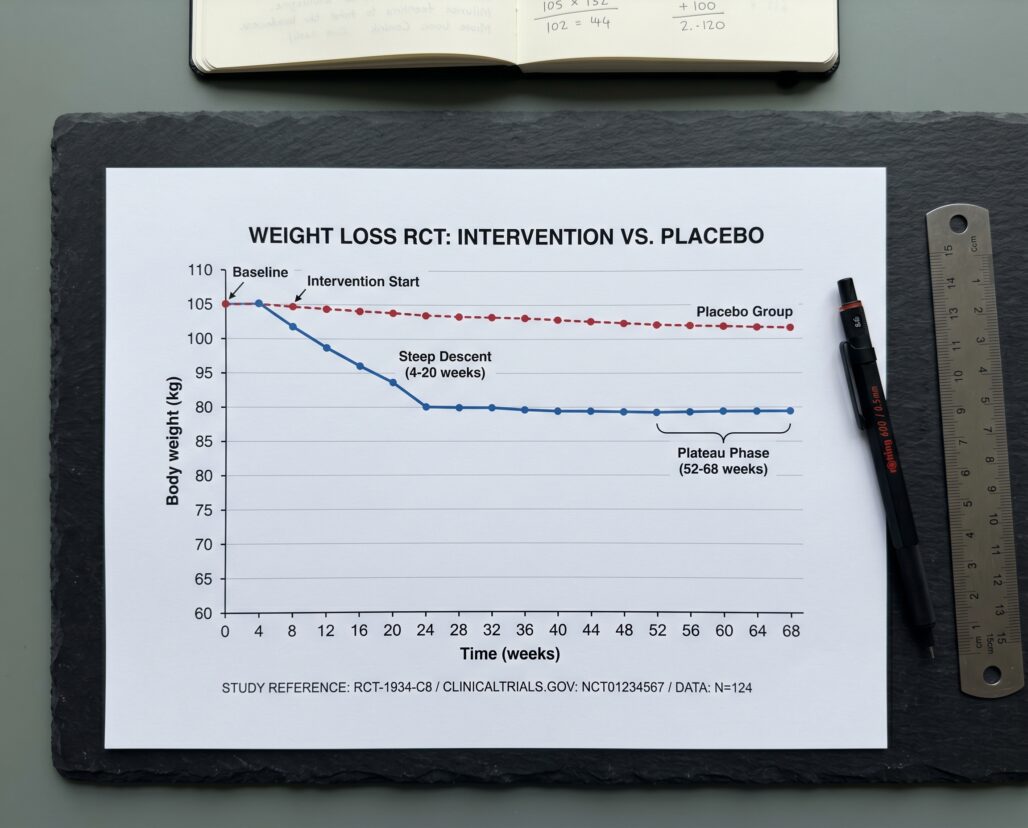
- GLP-1 agonists (semaglutide, liraglutide): Initial weight loss detectable by week 4; clinically meaningful loss by weeks 16-20; plateau typically between weeks 52-68 per STEP-1 data.
- Collagen peptides (oral): Skin elasticity improves detectably at 4-8 weeks in RCTs; wrinkle volume reduction is measurable at 4 weeks; neither effect is dramatic at the 4-week mark.
- Topical copper peptides (GHK-Cu): Human topical RCTs show skin improvements at 4-12 weeks; effect size is modest, not transformative.
- FDA-approved acute-use peptides: Bremelanotide works within 45 minutes of injection; insulin acts within 15-30 minutes (rapid-acting analogs, 10-20 minutes); glucagon reverses hypoglycemia within 10-15 minutes.
- Grey-market peptides (BPC-157, TB-500, GHRP-2, CJC-1295): No human RCT timeline data exists. Anecdotal reports and animal studies do not produce reliable onset or plateau estimates for humans.
Why "How Long" Depends Completely on What Outcome You Are Measuring
Timeline is not a fixed property of a peptide molecule. It is a relationship between a molecule, a biological target, and the specific outcome being tracked.
Semaglutide starts suppressing appetite within hours of the first dose. You will not see that on a scale for weeks because the starting dose (0.25 mg weekly) is deliberately sub-therapeutic, and weight loss requires a sustained caloric deficit, not a single skipped meal. If you measure "nausea," peak onset is weeks 1-4 during dose escalation. If you measure "body weight," meaningful change appears by weeks 8-12. If you measure "plateau," that is weeks 52-68. One drug, three very different timelines, all accurate.
Collagen peptides are digested into dipeptides and tripeptides, absorbed, and then need to stimulate fibroblast activity and matrix synthesis. The mechanism operates upstream of visible skin changes. Biomarkers like procollagen Type I synthesis are measurable at 8 weeks in an RCT, but your mirror reflects the downstream result, which accumulates more slowly. Expecting visible changes in two weeks is like expecting new muscle after one gym session.
Bremelanotide bypasses all of this by working acutely — it binds melanocortin receptors in the central nervous system and its effect window is measured in hours, not months. Understanding which timeline category your peptide falls into is the single most important calibration you can make.
GLP-1 Weight-Loss Timeline: Week by Week
The best timeline data for GLP-1 receptor agonists comes from the STEP trial program for semaglutide. STEP-1, a randomized double-blind placebo-controlled trial of 1,961 adults with obesity (BMI 30 or above, or 27 with at least one weight-related comorbidity), ran for 68 weeks and provides the most widely cited timeline benchmark in this class.
Key findings from STEP-1 (Wilding et al., NEJM 2021, PMID 33567185):
- Mean body weight change at week 68: -14.9% with semaglutide vs. -2.4% with placebo (treatment difference of 12.4 percentage points)
- Absolute weight loss: -15.3 kg with semaglutide vs. -2.6 kg with placebo
- 69.1% of semaglutide participants lost 10% or more of body weight
- 50.5% lost 15% or more
The STEP-1 extension study (PMID 35441470) — which followed participants for approximately one year after treatment ended — reported mean weight loss at 68 weeks of 17.3% in the semaglutide group, with participants regaining an average of 11.6 percentage points after treatment withdrawal, leaving a net loss of about 5.6% from baseline. The extension data makes an important practical point: the weight-loss timeline is also a weight-regain timeline if the drug is stopped.
Practical onset by phase:
- Weeks 1-4: Dose escalation (0.25 mg weekly). GI side effects peak here — nausea was the most common adverse event in STEP-1, described as transient and mild-to-moderate. 4.5% of semaglutide participants discontinued for GI reasons versus 0.8% with placebo.
- Weeks 4-16: Dose escalates toward the 2.4 mg maintenance level. Early measurable weight loss begins.
- Weeks 16-32: Steepest rate of weight loss for most participants, once at or near maintenance dosing.
- Weeks 52-68: Plateau. The curve flattens significantly. Stopping reverses most of the loss within about a year.
One critical compliance note for readers of childbearing potential: semaglutide is not recommended during pregnancy, and a pre-conception washout period of at least 2 months is advised before attempting conception, because the drug's half-life and potential embryofetal risks require time to clear.
Compounded semaglutide formulations — widely available online — have not been tested in any trial matching the STEP program. Timelines may differ from FDA-approved Wegovy due to formulation differences, and the FDA has explicitly warned about unapproved salt forms. See the semaglutide complete guide for the full regulatory picture.
Collagen Peptide Timeline: What the RCTs Actually Show
Oral collagen peptide supplements have more human RCT data than most supplements in this category, and the timelines are more conservative than product marketing suggests.
Proksch et al. (2013, PMID 23949208) ran a double-blind placebo-controlled trial of 69 women aged 35-55 on 2.5 g or 5.0 g of collagen hydrolysate (Verisol) daily for 8 weeks. Both dose groups showed statistically significant skin elasticity improvement vs. placebo by week 8 — detectable at week 4 but clearly significant by week 8. Women over 50 showed notably higher elasticity scores even at the 4-week post-treatment follow-up, suggesting a structural effect that continues building after supplementation ends. Skin moisture trends were positive but did not reach significance.
Proksch et al. (2014, PMID 24401291) ran a separate double-blind RCT of 114 women aged 45-65 on 2.5 g daily for 8 weeks. Results: a statistically significant 20% reduction in eye wrinkle volume detectable at 4 and 8 weeks, a 65% increase in procollagen Type I synthesis, and an 18% increase in elastin. Effects persisted at the 4-week post-treatment follow-up.
A 2019 systematic review (PMID 30681787) examined 11 randomized, placebo-controlled trials with 805 total patients using collagen hydrolysate doses of 2.5-10 g daily over 4-24 weeks. It found consistent improvements in skin elasticity, hydration, and dermal collagen density with good safety, while acknowledging variation in study quality.
Practical takeaway: Statistically measurable elasticity improvements appear at 4-8 weeks. Wrinkle reduction is measurable at 4 weeks under controlled conditions but will not be visible in a mirror. Twelve weeks is a realistic minimum for any consumer-perceptible change, and even then the effect is subtle.
Topical Peptide Timeline: GHK-Cu and Cosmetic Actives
Topical peptides — primarily used as cosmetic actives rather than drugs — operate on a different timeline structure than injectables or oral supplements. They need to penetrate skin, reach target cells, and trigger downstream synthesis pathways. That sequence takes weeks, not days.
The GHK-Cu copper peptide deep dive covers this molecule's mechanism in detail. For timeline purposes, the available human RCT data indicates:
- Early detectable changes in skin histology or patient-reported texture: 4-6 weeks in controlled topical studies
- Measurable improvement in fine lines, skin roughness, and photoaging markers: 8-12 weeks
- Maximum effect in the trials conducted: approximately 12 weeks of consistent daily application
Important calibration: GHK-Cu's human RCT database is smaller and less powered than the collagen supplement literature. Several trials are investigator-initiated with industry affiliation, and effect sizes in independent studies are more modest than brand-sponsored research. The biology — copper's role in lysyl oxidase activation and collagen crosslinking — is credible. The marketing timeline of "visible results in 7 days" is not.
Other topical peptides (Matrixyl/palmitoyl tripeptide-1, Argireline/acetyl hexapeptide-3) have similarly limited independent RCT bases. Where trials exist, timelines of 4-12 weeks for detectable changes are consistent across the category. No topical peptide active has demonstrated acute (same-day) visible effects in controlled trials.
FDA-Approved Acute-Use Peptides: Where Speed Actually Matters
Some FDA-approved peptide drugs work on the timescale of minutes, not weeks. Three are worth understanding for contrast:
Insulin (rapid-acting analogs): Lispro, aspart, and glulisine analogs begin lowering blood glucose within 10-20 minutes of subcutaneous injection, with peak effect at 30-90 minutes. Regular (human) insulin is slower, approximately 30 minutes to onset. The timing is why patients inject immediately before or with a meal.
Glucagon: Injectable or nasal glucagon raises blood glucose within 10-15 minutes in severe hypoglycemia. This is emergency reversal pharmacology, not supplementation.
Bremelanotide (Vyleesi): The only FDA-approved treatment for hypoactive sexual desire disorder (HSDD) in premenopausal women. The FDA label specifies administration at least 45 minutes before anticipated sexual activity, maximum one injection per 24 hours. Onset is approximately 45 minutes; duration is limited to hours, not persistent. The mechanism is central melanocortin receptor agonism — a fundamentally different target than metabolic or structural peptides. Nausea occurred in approximately 40% of phase III trial participants. It is a prescription drug, not a supplement.
Grey-Market Peptide Timeline Reality
This section needs to be read as a warning, not a guide.
BPC-157, TB-500 (thymosin beta-4), GHRP-2, GHRP-6, CJC-1295, Ipamorelin, MK-677, and the rest of the grey-market peptide catalog share one timeline characteristic: no human RCT timeline data exists for any of them.
The animal data for BPC-157 is substantial — rat models show accelerated tendon repair, gut mucosal healing, and improved healing metrics at timelines of days to weeks. Rat pharmacokinetics and human pharmacokinetics are not interchangeable. No dose-finding, no Phase I safety data, no Phase II efficacy data, no Phase III trial has ever been published for BPC-157 in humans under controlled conditions. "X days to feel it" claims circulating in bodybuilding forums and peptide vendor marketing have zero clinical grounding.
The same applies to TB-500, GHRP-2, GHRP-6, CJC-1295, and ipamorelin. GHRP-2 and GHRP-6 have limited Phase I pharmacokinetic data from the 1990s describing GH pulse patterns in healthy volunteers — but that data does not extend to outcome timelines for muscle growth, fat loss, or recovery. The others have essentially no published human trial data at all.
Before/after photos in grey-market peptide communities are uncontrolled anecdotes, not evidence. They have no baseline standardization, no control group, no blinded assessment, no exclusion of confounders (concurrent training, diet, other compounds), and are frequently created as paid testimonials by vendors or affiliates. The visual comparison you are looking at is not a timeline — it is a marketing artifact.
If you take any grey-market peptide and notice a change at "day 14," you cannot attribute that to the peptide rather than placebo effect, regression to the mean, concurrent lifestyle changes, or simply paying closer attention to your body once you started injecting something. The absence of a control condition makes the observation essentially uninterpretable.
Peptide Timeline Reference Table
| Drug / Peptide | Route | Onset (first detectable effect) | Clinically meaningful effect | Plateau or peak effect |
|---|---|---|---|---|
| Semaglutide (Wegovy) | SC injection, weekly | Week 4 (early weight loss) | Weeks 16-20 | Weeks 52-68 |
| Liraglutide (Saxenda) | SC injection, daily | Week 4-8 | Weeks 12-16 | Approximately week 52 |
| Collagen hydrolysate (oral, 2.5 g/d) | Oral | Week 4 (elasticity) | Week 8 | Week 8-12 |
| GHK-Cu (topical) | Topical | Week 4-6 | Week 8-12 | ~Week 12 |
| Bremelanotide (Vyleesi) | SC injection, PRN | 45 minutes | Same session | Duration: hours |
| Rapid-acting insulin analogs | SC injection | 10-20 minutes | 30-90 minutes | Single-dose, acute |
| Glucagon (hypoglycemia reversal) | SC/IM/nasal | 10-15 minutes | 15-30 minutes | Single-dose, acute |
| BPC-157 (grey-market) | SC injection | No human RCT data | No human RCT data | No human RCT data |
| TB-500 (grey-market) | SC injection | No human RCT data | No human RCT data | No human RCT data |
| GHRP-2 / GHRP-6 (grey-market) | SC injection | No human RCT data | No human RCT data | No human RCT data |
| CJC-1295 / ipamorelin (grey-market) | SC injection | No human RCT data | No human RCT data | No human RCT data |
Note: Compounded versions of FDA-approved peptides (compounded semaglutide, compounded bremelanotide) have not been tested in trials replicating the FDA-approved versions. Timelines may differ due to formulation differences in dosing, excipients, and purity. Do not assume equivalence.
Frequently Asked Questions
Why do I feel nothing after two weeks on a GLP-1?
Dose escalation. The starting dose of semaglutide (0.25 mg weekly for four weeks) is intentionally sub-therapeutic — its purpose is GI tolerance, not weight loss. Many people feel limited appetite suppression at this dose. The weight-loss dose (1.7 mg or 2.4 mg) is weeks away. Patience through the escalation schedule is part of the protocol, not a failure of the drug.
Can I speed up the collagen peptide timeline by taking more?
The Proksch 2013 trial found no statistically significant difference between 2.5 g and 5.0 g per day for skin elasticity outcomes. Higher dose did not produce faster results. More is not faster.
Why do my peptides from [online vendor] seem to work in 3 days when clinical trials show 4-8 weeks?
For grey-market peptides, the "effect" at day 3 is most likely placebo response, heightened body awareness, normal fluctuation, or an unrelated lifestyle change. For GLP-1 agonists at the sub-therapeutic starting dose, nausea is a real drug effect — but therapeutic appetite suppression takes weeks. For topical peptides, any perceived immediate glow comes from the emollients and humectants in the formulation, not the peptide's collagen-synthesis mechanism.
What happens to my weight if I stop semaglutide?
Per the STEP-1 extension data (PMID 35441470), participants who discontinued semaglutide regained an average of 11.6 percentage points of lost weight within approximately one year after stopping, leaving a net loss of only 5.6% from baseline. Weight management with GLP-1 agonists requires continued use to maintain results; the plateau does not persist after stopping. For collagen peptides, a similar principle applies: the Proksch 2013 data showed a lagged structural effect persisting at the 4-week post-treatment measurement, but without continued supplementation, collagen synthesis stimulus returns to baseline. Neither result is permanent on its own.
Conclusion
Realistic peptide timelines range from 45 minutes (acute FDA-approved drugs) to 4-8 weeks (measurable structural skin changes) to 52-68 weeks (GLP-1 weight-loss plateau). The most common mistake is applying the wrong benchmark — abandoning an evidence-backed treatment at week 4 because you expect week-68 results, or staying on a grey-market compound indefinitely because a forum post said "give it 30 days."
The table above reflects the most honest summary available from controlled trial data. For any compound not in it, or any outcome not tested in a human RCT, the only defensible answer is "we do not know" — and no quantity of before/after photos changes that.
All FDA-approved peptide drugs discussed here are prescription-only and require physician supervision. Timelines are population-level estimates from published trials and vary by individual.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The timelines and data presented are summaries of published research and should not be used to make personal health decisions. Consult a licensed healthcare professional before starting, stopping, or changing any medication or supplement. FDA-approved peptide drugs are prescription-only. Grey-market research peptides are not approved for human use and carry unknown safety risks.
