Affiliate disclosure: this article contains affiliate links. As an Amazon Associate, UsefulVitamins.com earns from qualifying purchases at no extra cost to you.
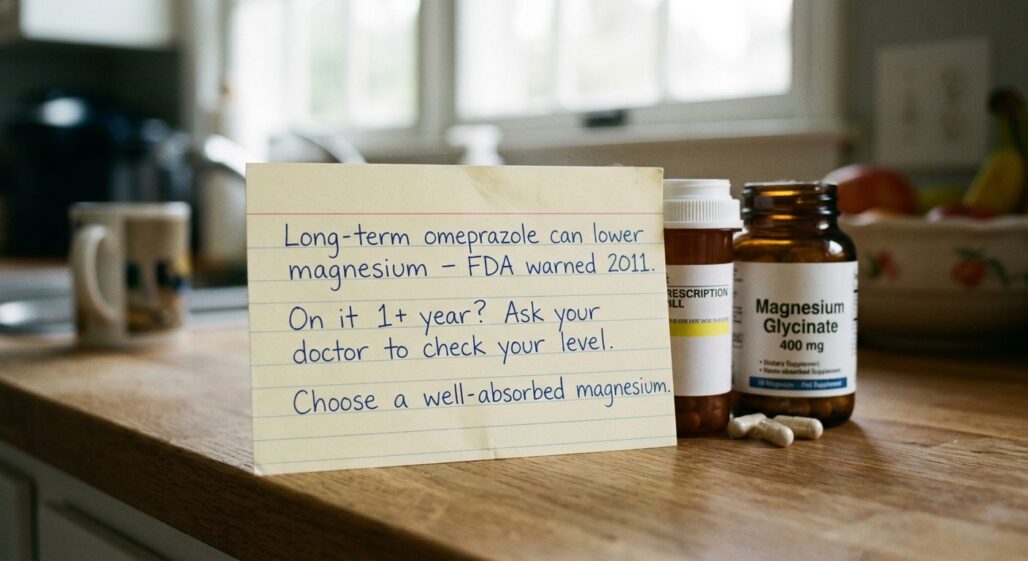
If you have been taking omeprazole for heartburn or reflux and read somewhere that it "drains your magnesium," the short answer is yes, long-term use can lower magnesium, and the FDA has formally warned about it since 2011. What that warning does not say is "panic and stop your pill." This article walks through how big the effect actually is, the mechanism in plain language, who is most at risk, and the practical steps that fix it without putting your reflux treatment at risk. The well-absorbed magnesium forms we would keep in our own family's cabinet are at the bottom, but the lab test comes first.
Before you decide

This is general nutrition information, not medical advice, and it is not a reason to change anything on your own. Never stop or lower a prescription PPI by yourself, because rebound acid and untreated reflux can be worse than a manageable mineral gap.
Some people need to be more careful than others. The highest-risk group is anyone on omeprazole for a year or more who also takes a diuretic, digoxin, or another drug that lowers magnesium. If that is you, the magnesium conversation with your prescriber is not optional housekeeping, it is part of safe long-term PPI use.
Call your doctor or pharmacist promptly if you notice muscle cramps or spasms, tingling, an irregular or racing heartbeat, unusual fatigue, or confusion. Severe low magnesium can cause seizures and dangerous heart rhythms, so symptoms plus a long PPI history are worth a same-week call, not a "mention it next year" item.
What the omeprazole-magnesium interaction actually is

Omeprazole is a proton pump inhibitor, or PPI. It works by shutting down the acid pumps in your stomach lining, which is exactly what makes it effective for reflux and ulcers. That same drop in stomach acid is what quietly interferes with magnesium absorption.
Your gut absorbs magnesium through two routes. Most of it crosses passively, but a fine-tuning active channel called TRPM6 (with its partner TRPM7) handles the rest, and that channel works best in a slightly acidic environment. A review in Gastroenterology Report describes how PPIs appear to impair this active transport, so less magnesium makes it from your food into your blood.
Two details matter here. First, this is an absorption problem, not a kidney problem, your kidneys are not dumping extra magnesium, your gut is taking in less. Second, this is slow. It is a months-to-years drift, not a day-one side effect, which is why most people never connect their cramps to a pill they have taken since 2019.
How big is the effect, really
This is where honest numbers matter more than scare headlines. The strongest summary we have is a 2019 meta-analysis in Medicine that pooled 16 observational studies and 131,507 patients. It found PPI users had a pooled adjusted odds ratio of 1.71 for low magnesium, roughly a 71% higher relative risk than non-users.
In raw terms, that worked out to about 19.4% of PPI users versus 13.5% of non-users showing low magnesium. A separate 2014 meta-analysis in PLoS One landed in the same zone with a pooled odds ratio near 1.78. So the signal is real and consistent, but the absolute jump is modest for most people.
The risk is also dose-dependent. The 2019 analysis found higher-dose PPI use carried about double the risk (odds ratio 2.13) compared with low-dose use. The real question is not "does omeprazole touch magnesium," it does, it is "are you in the slice of long-term, higher-dose, or co-medicated users where it becomes clinically meaningful."
The timing data tell the same story. The Gastroenterology Report review noted a median of about 5.5 years of PPI use before hypomagnesemia showed up, with cases ranging from two weeks to thirteen years. Years, not days, is the usual pattern.
Who is most at risk
Not every omeprazole user needs to worry equally. Magnesium status is a math problem of intake versus losses, and a few factors stack the deck.
Duration and dose come first. The longer and higher the PPI dose, the bigger the absorption hit. A few weeks of over-the-counter omeprazole for a flare is a very different situation from daily 40 mg for several years.
Co-medications are the multiplier. The FDA's 2011 safety communication singled out people who also take diuretics or digoxin, because diuretics increase magnesium loss and low magnesium makes digoxin more dangerous to the heart. That combination is the one clinicians watch most closely.
Diet is the quiet baseline. The average Western diet runs below the magnesium target, and the NIH Office of Dietary Supplements sets the RDA at 400 to 420 mg for adult men and 310 to 320 mg for adult women, with a meaningful share of US adults coming in under that even before any drug effect. If your diet was already borderline, omeprazole pushes a near-empty tank closer to the warning light. Older adults, heavy alcohol use, and chronic diarrhea or malabsorption add further losses on top.
What to do about it (the practical part)
Here is the part most articles skip in favor of fear. The fix is layered, and almost none of it involves quitting your PPI unilaterally.
Step one is a blood test, not a supplement. Blood work changes the question, without it you are guessing whether you are actually low. Ask your doctor for a serum magnesium level, and ideally a repeat after a few months on long-term therapy. One honest caveat: serum magnesium can read normal even when body stores are running down, so your symptoms still count.
Step two is food first. It is the cheapest intervention you have. Pumpkin seeds, almonds, spinach, black beans, and whole grains are dense magnesium sources, and shifting your plate can close a good part of a typical intake gap before any pill enters the picture.
Step three, if a supplement is warranted, is choosing the right form and spacing it sensibly. The average US diet covers only part of the magnesium RDA, so a 200 to 300 mg supplement usually closes a gap rather than overshooting it. There is a difference between the dose that fixes a real shortfall and the dose that just stacks up and gives you loose stools.
One important honesty point from the literature: in more severe cases, oral magnesium alone often is not enough while the PPI continues, because the drug keeps blunting absorption. The Gastroenterology Report review describes cases where levels only normalized after the PPI was reduced, switched, or stopped under supervision, sometimes within a few weeks of the change. That decision belongs to your prescriber, who may consider a lower dose, an H2 blocker like famotidine, or intermittent use.
If you are juggling omeprazole, a magnesium supplement, and other prescriptions, our companion app StackMyMed can help you log the stack and flag this kind of conflict, though it helps you spot and space things, it is not a replacement for your pharmacist's review.
It is also worth knowing this is not the only nutrient omeprazole touches; long-term PPI use is linked to lower B12 too, which we cover in our guide to omeprazole and vitamin B12 deficiency.
What to look for when buying a magnesium supplement
If your doctor agrees a supplement makes sense, the form matters more than the milligram number on the front of the bottle. The cheapest, most common form, magnesium oxide, is also the worst absorbed.
A classic study on the bioavailability of US magnesium preparations measured magnesium oxide at only about 4% fractional absorption, meaning the large majority passes through unused and mostly acts as a laxative. Organic forms like citrate, lactate, and chloride absorbed substantially better in the same line of research.
For an absorption problem caused by a PPI, that gap is the whole point, you want the magnesium that actually crosses the gut wall, not the one that races through it. Here is how the common forms compare for this specific use.
| Form | Absorption | Gut tolerance | Best for |
|---|---|---|---|
| Glycinate | High | Gentlest, minimal laxative effect | Daily maintenance on a long-term PPI |
| Citrate | High | Good, mild laxative at higher doses | Best cost-per-absorbed-mg if your gut tolerates it |
| Oxide | Low (about 4%) | Often loosens stools | The form to skip for correcting a PPI-driven gap |
A reasonable default is magnesium glycinate for the gentlest daily option, or citrate if you want the most absorbed magnesium per dollar and your stomach tolerates it. Look for a third-party verified product (USP Verified, NSF, or ConsumerLab approved) so the label reflects what is in the capsule. For the deeper form-by-form breakdown, see our complete guide to magnesium and our pick for the best magnesium supplement overall.



As an Amazon Associate, UsefulVitamins.com earns from qualifying purchases at no extra cost to you. We only recommend products supported by published research or third-party testing.
When to see a clinician
Some situations move this from a supplement question to a medical one. Get evaluated promptly, not eventually, if you have low-magnesium symptoms plus a long PPI history.
Red flags include persistent muscle cramps or spasms, numbness or tingling, tremor, an irregular or pounding heartbeat, unusual fatigue, or confusion. These overlap with low calcium and low potassium, which often ride along with low magnesium, so this is a blood-panel conversation, not a self-diagnosis.
Two scenarios deserve same-week attention: you also take a diuretic or digoxin, or your symptoms are escalating. Bring your full medication and supplement list to the visit so your clinician can see the whole stack, including over-the-counter omeprazole you might not think to mention. For a broader view of which pills and nutrients clash, our ultimate guide to drug-supplement interactions and the drug-supplement interaction checker are good next stops.
FAQ
Does short-term omeprazole lower magnesium?
Short courses are very unlikely to matter. The risk in the literature clusters around long-term use, with hypomagnesemia typically appearing after about a year and often much longer.
Will taking a magnesium supplement fully fix it while I stay on omeprazole?
Sometimes, for milder gaps. But in more pronounced cases the literature shows oral magnesium alone does not normalize levels while the PPI keeps blunting absorption, which is why a clinician may adjust the drug rather than just add a pill.
Should I switch to an H2 blocker like famotidine?
That is a conversation for your prescriber, not a self-swap. H2 blockers reduce acid by a different route and are not linked to the same magnesium problem, so they are one option a doctor may weigh if your reflux can be controlled with less acid suppression.
Does omeprazole affect any other nutrients?
Yes. Long-term use is also associated with lower vitamin B12 and can affect calcium and iron absorption, since all of these depend partly on stomach acid.
How much magnesium should I take?
There is no one answer without your lab values, but supplemental magnesium is generally kept to about 350 mg per day from supplements unless a doctor directs otherwise, because higher amounts mostly cause diarrhea. Let your magnesium level and your diet set the dose.
The bottom line on omeprazole and magnesium
Omeprazole really can lower magnesium, the FDA confirmed it in 2011, and the meta-analyses put the relative risk around 70% higher in long-term users. But the absolute effect is modest for most people, it builds over years, and it hits hardest in those on high doses, long durations, or magnesium-lowering co-medications like diuretics and digoxin. This is a manageable interaction, not a reason to abandon needed reflux treatment.
Next steps:
- Ask your doctor for a serum magnesium check if you have been on omeprazole for a year or more, especially with cramps, palpitations, or a diuretic or digoxin in your stack.
- Eat more magnesium-rich food first, then add a well-absorbed supplement (glycinate or citrate, not oxide) only if a gap remains.
- Never stop or change your PPI on your own; bring your full pill list to your clinician and let your labs guide the plan, see our how we review supplements process for how we weigh this evidence.
As an Amazon Associate, I earn from qualifying purchases. Product recommendations are based on real reviews and independent research.
This article is for informational purposes and not medical advice. Proton pump inhibitors and supplements can interact with each other and with health conditions. Consult a licensed physician or pharmacist before starting, stopping, or changing any medication or supplement, particularly if you are pregnant, nursing, taking other prescription medications such as diuretics or digoxin, or managing a chronic condition. Reviewed by the UsefulVitamins Editorial Team.