The phrase "peptide stack" shows up in two completely different universes, and the gap between them is wider than most people realize. In a hospital formulary meeting, a peptide "stack" means a deliberately designed, FDA-evaluated drug combination with documented pharmacokinetic interactions, dosing thresholds, and adverse-event monitoring protocols built over years of trials. On a bodybuilding forum, "stack" means a list of compounds assembled from animal-model studies, vendor copy, and other users' anecdotal logs. Both groups use the same word. The word means very different things. If you want to evaluate whether any given peptide combination is evidence-based or speculative, that distinction is the most important place to start — because the gap in risk profile between the two categories is significant.
Summary
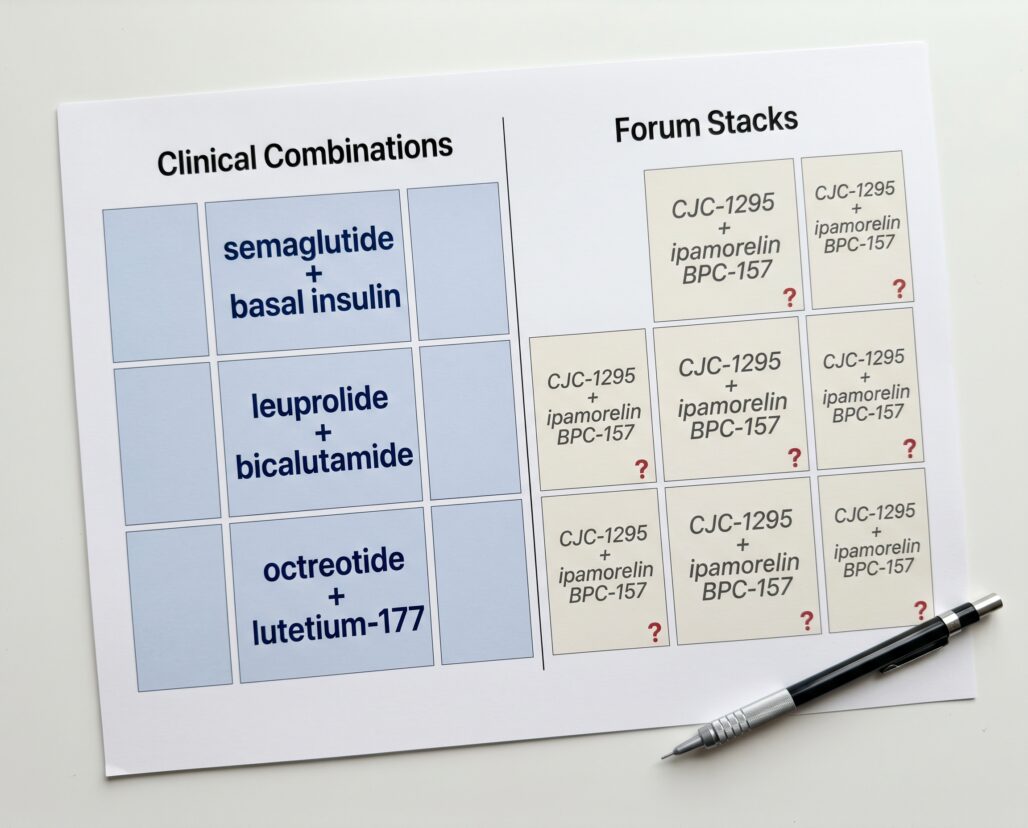
What "stacking" means in this article: Any deliberate combination of two or more peptide compounds used simultaneously to achieve a therapeutic or performance outcome.
Clinical combinations covered below: Semaglutide added to basal insulin for type 2 diabetes; leuprolide combined with an antiandrogen for advanced prostate cancer; octreotide combined with radioligand therapy for neuroendocrine tumors.
Grey-market forum stacks covered below: CJC-1295 combined with ipamorelin; BPC-157 combined with TB-500; GHRPs layered with exogenous growth hormone.
One-sentence bottom line on evidence: Every clinical combination in this article is backed by randomized controlled trial data and FDA-evaluated prescribing information. Not a single grey-market forum stack has a published randomized controlled trial testing the specific combination in humans.
If you are currently using or considering an unapproved peptide combination: The conversation belongs with a licensed physician, not a forum moderator. No responsible interpretation of the available evidence supports self-managing multi-compound peptide regimens outside medical supervision.
What "Stacking" Actually Means in Clinical Pharmacology
Clinical pharmacologists combine drugs when evidence shows the combination produces a benefit — better efficacy, fewer side effects, improved tolerability — that neither drug achieves alone. That evidence is generated through trials: first pharmacokinetic studies to understand how the drugs interact at the level of absorption, distribution, metabolism, and excretion, then efficacy trials comparing the combination against each monotherapy, then post-market safety surveillance.
Adding any second compound to a first creates the possibility of altered receptor dynamics, shifted half-lives, changed clearance rates, and new adverse-event patterns that did not exist with either agent alone. Predicting those changes requires human data, not biological rationale alone.
Forum stacks operate on a different logic: Compound A acts on pathway X. Compound B acts on pathway Y. Pathways X and Y are related. Therefore combining A and B produces synergistic effects. That reasoning sounds scientific. It is not the same as tested. Synergy can be real; it can also produce unexpected toxicity when pathways interact in ways animal-model data did not anticipate. Combining unverified peptides multiplies the unknowns rather than dividing the risk.
Clinical Peptide Combinations: What FDA-Approved Medicine Actually Uses
Semaglutide Added to Basal Insulin in Type 2 Diabetes
The SUSTAIN 5 trial (PMID: 29688502) tested subcutaneous semaglutide at 0.5 mg and 1.0 mg once weekly added to stable basal insulin therapy across 397 patients with inadequately controlled type 2 diabetes over 30 weeks. Semaglutide at 1.0 mg reduced HbA1c by 1.8 percentage points versus 0.1 points on placebo (p less than 0.0001), with a 6.4 kg weight reduction versus 1.4 kg on placebo. Severe or confirmed hypoglycemic episodes occurred in 25 patients on the 1.0 mg dose versus 13 on placebo — a numerically higher rate that did not reach statistical significance in this trial but that prescribers monitor closely in clinical practice.
A subsequent meta-analysis of seven RCTs covering 2,354 patients (PMID: 39892787) confirmed the pattern: mean HbA1c reduction of 1.17 percentage points, mean weight loss of 5.99 kg, no statistically significant increase in hypoglycemia risk (RR 1.46, p = 0.13), but elevated gastrointestinal adverse events across the combination arm.
Adding a GLP-1 receptor agonist to basal insulin carries a lower hypoglycemia risk than adding a sulfonylurea or rapid-acting insulin, because semaglutide's glucose-lowering mechanism is glucose-dependent. Combining any glucose-lowering agents still requires active management: regular monitoring, insulin dose adjustment, and clear patient instructions. Simultaneously adding a sulfonylurea to this combination substantially increases hypoglycemia risk and requires close physician oversight. This is not a combination to initiate or adjust without a physician managing the protocol.
The trajectory is toward tighter integration: the COMBINE 3 trial (PMID: 40482670) tested IcoSema — a once-weekly fixed-ratio combination of basal insulin icodec and semaglutide — against daily basal-bolus therapy, achieving non-inferior glycemic control with superior weight reduction and lower hypoglycemia rates.
Leuprolide Combined with Antiandrogens in Advanced Prostate Cancer
Combined androgen blockade — a GnRH agonist such as leuprolide paired with a first-generation antiandrogen such as flutamide or bicalutamide — has been the subject of systematic review and meta-analysis since the 1990s. A comprehensive evidence report examining MEDLINE, CANCERLIT, and EMBASE databases from 1966 through 1998 (PMID: 11098244), covering the full body of RCT evidence at the time, found no statistically significant 2-year survival difference between combined androgen blockade and monotherapy. The 5-year analysis showed a statistically significant but clinically modest survival advantage favoring the combination, with the important caveat that adverse effects leading to therapy withdrawal were more common in the combination arm.
Combined androgen blockade remains a standard option for specific presentations of advanced prostate cancer. The point is not that the combination is ineffective — it is that even a regimen with thirty years of human trial data, FDA-approved components, and well-characterized adverse-event profiles requires oncologist-led decision-making: evaluation of disease stage, cardiovascular risk (GnRH agonists are associated with insulin resistance and dyslipidemia), and individual tolerability. Flutamide adds hepatotoxicity monitoring; bicalutamide adds a different profile. If that level of clinical management is required for a thoroughly studied combination, combinations with essentially no human data operate in a categorically different risk environment.
Octreotide and Radioligand Therapy in Neuroendocrine Tumors
Somatostatin receptor-positive neuroendocrine tumors represent a third clinical use case where a peptide — octreotide or lanreotide — is used in deliberate combination with another therapeutic modality. In PRRT (peptide receptor radionuclide therapy) using lutetium-177 dotatate (Lutathera), the radiolabeled peptide targets somatostatin receptors on tumor cells for localized radiation delivery. Long-acting somatostatin analogues are typically continued during and after treatment both for symptom control and because there is evidence they reduce receptor downregulation that could otherwise diminish PRRT uptake.
This combination was evaluated in the NETTER-1 phase 3 randomized trial and represents a textbook example of what rigorous peptide combination development looks like: a specific FDA-approved indication, defined patient selection criteria, and mandatory radiation safety, renal, and hematologic surveillance managed within academic oncology settings.
Grey-Market Forum Stacks: What the Evidence Actually Shows
CJC-1295 Combined with Ipamorelin
This is probably the most commonly discussed grey-market peptide stack. The biological rationale holds: CJC-1295 is a GHRH analog acting on the hypothalamus-pituitary axis, and ipamorelin is a selective ghrelin receptor agonist. They act through complementary but distinct receptors to stimulate growth hormone release, and animal data — primarily murine models — shows additive effects on muscle tissue in some experimental conditions (PMID: 41476424).
What does not exist is a published randomized controlled trial testing the specific combination in humans. A 2026 review of injectable peptide therapies for orthopaedic and sports medicine physicians (PMID: 41476424) noted that "CJC-1295 combined with ipamorelin showed significantly improved maximum tetanic tension in murine models" and immediately clarified that human orthopaedic data remain absent. A separate 2026 Sports Medicine review (PMID: 41966639) covering both compounds described human safety data for each as "scarce," with potential for serious harm. A concurrent review in the Journal of the American Academy of Orthopaedic Surgeons (PMID: 41490200) labeled both as "preclinical only" and stated plainly that "although preclinical studies are promising, there is a current lack of clinical trials."
Neither CJC-1295 nor ipamorelin is FDA-approved. Both are on the WADA prohibited list under S2.2.4. The combination has no established human dosing, no published pharmacokinetic interaction data in humans, no defined monitoring protocol, and no safety profile derived from human subjects.
BPC-157 Combined with TB-500
The BPC-157 plus TB-500 (thymosin beta-4) stack circulates heavily in injury-recovery and performance communities. The rationale — one peptide for tissue healing, one for angiogenesis and inflammation — is borrowed from animal experiments. Neither compound has completed a phase 2 or phase 3 human clinical trial. The Sports Medicine review (PMID: 41966639) places both in the "primarily animal evidence / scarce human safety data / potential for serious harm" category. TB-500 is prohibited in sports competition. BPC-157 has been placed by the FDA on its list of bulk drug substances presenting significant safety risks for compounding, meaning it cannot legally be included in compounded medications in the United States — not because it has been proven harmful in humans, but because insufficient human data exists to establish that it is safe.
The combination of the two compounds has no published human data whatsoever. Combining two compounds each with individually uncharacterized human pharmacology does not average their unknown risk profiles — it creates a new, even less understood risk profile.
GHRPs Stacked with Exogenous Growth Hormone
Some forum protocols layer GHRP-2 or GHRP-6 on top of exogenous recombinant human growth hormone (rhGH). The logic — that GHRPs stimulate pituitary GH release while exogenous GH provides a direct substrate boost — ignores a physiological feedback mechanism: supraphysiologic exogenous GH down-regulates endogenous GH secretion through somatostatin upregulation, which reduces the receptor responsiveness that GHRPs depend on. The expected synergy may be partially or fully negated by the very biology it is attempting to exploit. More critically, rhGH is FDA-approved for specific pediatric and adult indications under physician supervision with regular IGF-1 monitoring, because chronic supraphysiologic GH and IGF-1 exposure is associated with insulin resistance, joint pain, carpal tunnel syndrome, and potentially increased oncologic risk in specific populations. Adding a GHRP on top escalates dosing uncertainty in a system that requires careful monitoring even in its approved forms.
Why Combining Unverified Peptides Multiplies Risk
Combination pharmacology in the absence of human data creates risk in at least three distinct ways.
Interaction unknowns. Two compounds acting on related receptors can produce unexpected crosstalk, altered hormone feedback loops, or changed clearance rates that neither produces alone. Animal pharmacokinetics do not reliably predict human pharmacokinetics.
Dose uncertainty compounds. Neither compound in most grey-market stacks has an established human dose from phase 1 trials. Stacking two compounds with individually unknown dose-response relationships leaves the interaction space entirely uncharted.
Manufacturing risk is additive. Grey-market peptides are not manufactured to pharmaceutical-grade sterility, potency, and purity standards. Each additional vial from a different vendor or batch expands the surface area for contamination, mislabeling, or incorrect concentration.
No published randomized controlled trial has tested CJC-1295 plus ipamorelin in humans. No published randomized controlled trial has tested BPC-157 combined with TB-500 in humans. No published randomized controlled trial has tested any GHRP combined with exogenous rhGH as a deliberate protocol in healthy adults. That is a fundamental gap in the evidence that forum anecdote cannot fill.
How to Talk to Your Prescriber About Combination Therapy
If you are interested in peptide therapy — for metabolic health, injury recovery, or hormone optimization — the path to an evidence-based conversation with a physician runs through specific, answerable questions. These are worth knowing before you book an appointment.
Ask for the specific indication. "Is there an FDA-approved use for this combination, or is this off-label? If off-label, what is the published evidence for this application?"
Ask about the monitoring protocol. Any legitimate combination peptide therapy should come with defined monitoring: which labs, how frequently, what thresholds trigger dose adjustment or discontinuation. A prescriber who cannot answer this question is prescribing without a safety net.
Ask about drug interactions. If you take any other medications — including supplements — ask specifically whether the proposed peptide therapy interacts with them. GLP-1 receptor agonists slow gastric motility and can alter the absorption timing of oral medications. GnRH analogues affect gonadal steroid levels that interact with a wide range of systems. A responsible prescriber runs this check before prescribing.
Bring the forum protocol if you have one. Showing a physician what you were considering often produces a more useful conversation than asking generically about peptides. The physician can explain precisely where the protocol's assumptions diverge from human trial data — and may offer a supervised alternative that addresses the same goal.
Frequently Asked Questions
Are there any grey-market peptide stacks with strong human evidence?
No combination of currently unapproved peptides has published phase 2 or phase 3 randomized trial data supporting use in healthy adults. The human evidence gap is consistent across CJC-1295, ipamorelin, BPC-157, TB-500, and similar grey-market compounds.
Can I ask a doctor to prescribe CJC-1295 plus ipamorelin?
A physician can prescribe off-label therapies if they judge the clinical rationale to be sound and the patient is informed of the evidence limitations. What a licensed 503A or 503B compounding pharmacy cannot do is compound CJC-1295 or ipamorelin for human use under current FDA bulk drug substance policy. The regulatory and evidence picture for this stack is not favorable.
Is semaglutide plus insulin dangerous?
The combination is well-studied and can be appropriate for specific patients with inadequately controlled type 2 diabetes. It requires physician management, careful insulin dose adjustment, and glucose monitoring. The combination is not appropriate for self-initiation and carries specific contraindications that only a prescriber evaluating your full medical history can assess. Combining semaglutide with insulin and a sulfonylurea simultaneously substantially increases hypoglycemia risk and should only occur under close medical supervision.
Are "peptide clinics" prescribing these stacks safely?
Quality varies widely. Critical markers: full medical history and examination before prescribing, a documented monitoring protocol, a licensed 503A or 503B pharmacy supplying the product, and a prescriber who can articulate the evidence basis for the specific combination. A clinic unable to answer those questions concretely is not operating to a standard that protects patients.
My forum stack "worked" — what does that mean?
Self-reported outcomes can reflect a real drug effect, placebo response, concurrent lifestyle changes, or confirmation bias. None of those interpretations require documented safety for the combination used. Personal experience is not a substitute for population-level safety trials.
Conclusion
The clinical peptide combinations used in modern medicine — GLP-1 receptor agonists added to basal insulin, leuprolide plus antiandrogen blockade in prostate cancer, somatostatin analogues combined with radioligand therapy — share several characteristics: they were tested in randomized controlled trials, the prescribing information documents their interactions and adverse effects, and physician supervision is built into every stage of their use. Those characteristics are not bureaucratic formalities. They are the mechanism by which medicine learns what is actually safe.
Grey-market peptide stacks lack all of those characteristics. The biological reasoning behind CJC-1295 plus ipamorelin or BPC-157 plus TB-500 is not incoherent. The evidence that the specific combination is safe and effective in humans does not exist. That gap cannot be bridged by animal data, vendor marketing, or forum aggregation of n=1 reports. Combining two compounds with individually uncharacterized human pharmacology does not produce a known outcome — it produces a larger unknown.
If you are interested in peptide therapy for any clinical purpose, the conversation that can be grounded in evidence runs through a physician and a pharmacy under regulatory oversight. The version that runs through a forum thread and an offshore vendor operates in a risk environment the published literature does not support. Understanding which version you are in is the starting point for an informed decision about whether peptides are appropriate for your situation.
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Consult a qualified healthcare professional before starting, stopping, or changing any medication or supplement regimen. The regulatory and clinical information cited reflects sources available as of the publish date and may change as new evidence emerges.
