If you have an autoimmune condition and a wellness account told you a peptide will "rebalance" your immune system, the honest answer is this: nothing on the consumer market carries FDA approval for an autoimmune indication, and immune modulation done wrong can make autoimmune disease considerably worse. Autoimmune disease is not a case of an immune system that needs a general boost — it's a case of misdirected immune activity attacking the body's own tissue. Stimulating or shifting that system without precise, monitored intervention is not the same as fixing it. This article covers what the research actually says about peptides and autoimmunity, which compounds are being studied and why, where the evidence stops, and why the established treatment landscape exists for reasons that matter to your long-term health.
Quick Summary
Peptides studied in autoimmune contexts include thymosin alpha-1, BPC-157, and KPV. None are FDA-approved in the United States for any autoimmune indication. Most evidence comes from animal models or small preliminary human trials. Low-dose naltrexone is frequently mentioned alongside peptides in this space but is not a peptide — it is a small-molecule opioid antagonist, and the two categories are medically distinct. Approved autoimmune therapies including DMARDs, biologics, and JAK inhibitors carry documented mechanisms and monitored risk profiles that grey-market peptides cannot match. Replacing or skipping prescribed therapy to self-experiment with unregulated compounds carries genuine risk of disease flare, joint destruction, organ damage, and in some conditions, permanent disability.
Why People With Autoimmune Conditions Turn to Peptides
The appeal is understandable. Autoimmune disease is exhausting beyond the symptoms. Treatment calendars are demanding: regular bloodwork, infusion appointments, monthly injections, periodic imaging. Side effect profiles for DMARDs and biologics are real, and many patients live with residual symptoms even on optimized therapy — partial remission, not full.
Against that backdrop, a social-media claim that a peptide will "rebalance" the immune system sounds attractive. The language of wellness content is also strategically vague: "modulating" immunity, "supporting" immune homeostasis, "reducing systemic inflammation." These phrases gesture at mechanisms without citing evidence that would let you evaluate them.
Two dynamics push people further in this direction. Compounding pharmacies and grey-market vendors grew far more visible post-pandemic on the back of GLP-1 interest, and the same distribution channels that supply compounded semaglutide also supply peptides that have never cleared a phase 2 human trial. The [what-are-peptides] framing of peptides as "naturally occurring" and "body-identical" also creates the impression they are inherently safe — an impression that collapses when you look at what autoimmune immune modulation actually requires clinically.
What Is Actually Being Researched
Thymosin Alpha-1: The Most Studied Peptide in Autoimmunity
Thymosin alpha-1 (Ta1) is a 28-amino-acid peptide derived from thymosin fraction 5, a thymic extract that has been studied since the 1970s. Of all the peptides discussed in autoimmune contexts, it has the most substantial human research base.
A 2024 systematic review published in Alternative Therapies in Health and Medicine (PMID 38308608) examined more than 11,000 human subjects across 30-plus clinical trials. The authors concluded that Ta1 "emerges as a well-tolerated and effective immune modulator" with applications in infectious disease, cancer, and — more selectively — autoimmune conditions. Patients with systemic lupus erythematosus, rheumatoid arthritis, and psoriatic arthritis showed significantly lower serum Ta1 levels than healthy controls in a 2016 study (PMID 27350088), suggesting a possible pathophysiological role rather than a simple deficiency to be corrected.
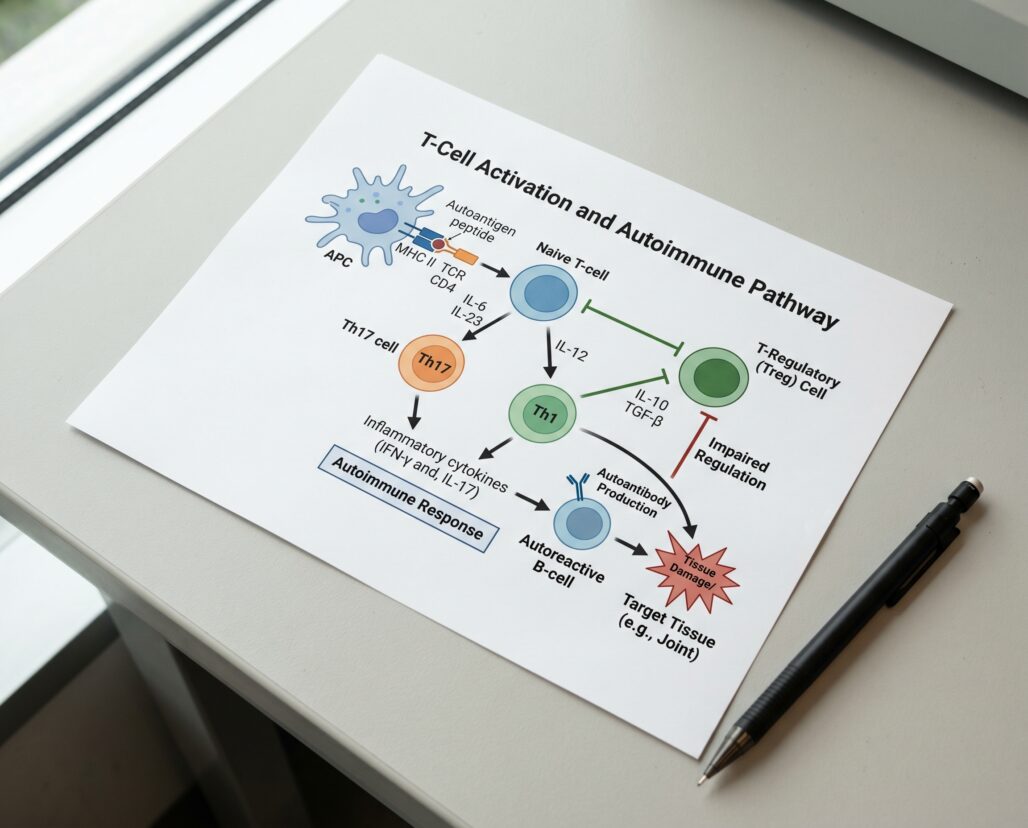
The immune mechanism is the critical complication here. Ta1 acts primarily by enhancing regulatory and tolerogenic pathways — promoting dendritic cell activity, modulating T-helper cell balance, and supporting regulatory T cell (Treg) populations. In a 2020 study (PMID 32817121), Ta1 prevented immune-related adverse events from checkpoint inhibitor therapy by restoring immune tolerance — a distinct goal from stimulating immune activity broadly.
FDA status callout: The FDA restricted thymosin alpha-1 from compounding pharmacy use in 2023, placing it on the list of substances that may not be compounded under 503A regulations. The compound is not approved in the United States as a drug or dietary supplement for any indication. It is approved in roughly 40 other countries under the brand name Zadaxin primarily for hepatitis B and as an immune adjunct in cancer care, but those approvals do not transfer to U.S. autoimmune use. Self-obtaining Ta1 from grey-market sources means receiving a compound with no verified sterility, no confirmed dosage, and no pharmaceutical-grade manufacturing guarantee.
BPC-157: Promising in Animals, Absent in Autoimmune Human Trials
BPC-157 (Body Protection Compound 157) is a synthetic pentadecapeptide derived from a protein found in gastric juice. It has generated interest for tissue healing, gut protection, and anti-inflammatory effects — but almost entirely in rodent models.
The research base for BPC-157 and autoimmune conditions specifically is thin to nonexistent. Animal studies have shown cytoprotective and anti-inflammatory effects in models of organ injury and GI inflammation, including a 2025 rat study (PMID 40005408) demonstrating reduced organ damage from ischemia-reperfusion injury. The mechanism appears to involve nitric oxide modulation, growth hormone receptor interaction, and reduction of oxidative stress markers.
FDA status callout: BPC-157 has no FDA approval for any indication in humans. The FDA has specifically issued warning letters to vendors marketing BPC-157 as a supplement or research chemical for human use. There are no completed phase 2 or phase 3 human trials for BPC-157 in any autoimmune condition as of early 2026. The compound is popular on bodybuilding and biohacking forums, but popularity is not a proxy for clinical evidence. Translating rodent results to human autoimmune biology — a process where the immune system is chronically dysregulated, often medicated, and highly individual — requires controlled human trials that do not yet exist.
KPV: Anti-Inflammatory Tripeptide With Colitis Data, But Only in Animals
KPV is a tripeptide (lysine-proline-valine) derived from the C-terminal sequence of alpha-melanocyte-stimulating hormone. Its main research territory is intestinal inflammation and colitis models.
A 2008 study (PMID 18061177) showed KPV acts via the PepT1 transporter in immune and epithelial cells to inhibit NF-kappaB activation and reduce pro-inflammatory cytokine secretion. Oral administration reduced DSS- and TNBS-induced colitis in mice. Subsequent work (PMID 28143741, 2017) used hyaluronic acid-functionalized nanoparticles to deliver KPV to the colon with superior efficacy at much lower doses than free peptide.
The finding is mechanistically interesting: NF-kappaB inhibition is a shared pathway in Crohn's disease and ulcerative colitis. The problem is that every study above used murine models. No published human trials of KPV as a standalone anti-inflammatory exist in inflammatory bowel disease. The gap between a mouse colitis model and a human patient on immunosuppressive therapy for Crohn's disease is not bridgeable by enthusiasm.
FDA status callout: KPV has no FDA approval for any indication. It is not classified as a drug or dietary supplement with recognized safety data in humans.
Low-Dose Naltrexone: Not a Peptide, But Constantly Conflated With One
Low-dose naltrexone (LDN) deserves its own section because it is routinely mentioned in the same conversations as peptides, and that conflation is a source of real confusion.
LDN is not a peptide. It is a small-molecule opioid antagonist — specifically, a mu-opioid receptor antagonist originally approved at standard doses (50 mg) for opioid and alcohol use disorder. At doses of 1.5 to 4.5 mg (roughly 10% of the approved dose), it appears to function differently, intermittently blocking opioid receptors in ways that upregulate endogenous opioid production and modulate glial cell activity. The anti-inflammatory effect is thought to involve toll-like receptor 4 (TLR4) blockade and reduced microglial activation.
Human research exists. A 2018 review (PMID 29377216) found LDN demonstrated safety and tolerability in multiple sclerosis, fibromyalgia, and Crohn's disease. A 2020 update (PMID 32845365) documented symptom reduction in several inflammatory conditions. Most LDN autoimmune trials remain small and short-duration, without active comparators against standard-of-care therapies.
LDN is prescribed off-label by some physicians and is not FDA-approved for autoimmune conditions. It is a legitimate subject of ongoing research. But calling it a peptide is medically incorrect, and the conflation matters because it lends borrowed credibility to the peptide category at large — a category where the human evidence base is far thinner.
Why "Modulating Immunity" With Grey-Market Peptides Is High-Risk
The wellness framing of immune modulation implies a gentle, corrective nudge toward homeostasis. The clinical reality of autoimmune disease is more volatile than that framing suggests.
Autoimmune conditions involve a fundamentally dysregulated immune response. In rheumatoid arthritis, immune cells attack the synovial lining of joints. In lupus, immune complexes deposit in kidneys, skin, and blood vessels. In multiple sclerosis, myelin sheaths surrounding nerve fibers are degraded. These are not situations where the immune system needs a general tune-up — they require targeted suppression or redirection of specific immune pathways, monitored with blood panels, imaging, and regular clinical evaluation.
Stimulating immune activity in this context can trigger flares. A peptide that broadly enhances T-cell activity or increases cytokine signaling does not distinguish between the regulatory pathways you want to support and the pathogenic pathways driving tissue damage. Thymosin alpha-1, the most research-backed option on this list, primarily works through tolerogenic and regulatory mechanisms — but those mechanisms are dose-sensitive, context-dependent, and have been studied in monitored clinical settings, not in self-administration by patients who obtained the compound from an international online vendor.
The purity problem is equally serious. Regulatory-quality Ta1, BPC-157, or KPV requires sterile synthesis, independent assay verification, and controlled storage. Grey-market peptides from unregulated manufacturers have shown contamination with heavy metals, bacterial endotoxins, and mis-dosed active ingredient in third-party testing. Injecting a contaminated compound into an already-dysregulated immune system is not modulation — it is an infection risk.
Critical safety warning: Do not stop or replace prescribed autoimmune therapy with peptides. Discontinuing a DMARD or biologic without rheumatologist supervision can trigger disease flare and irreversible damage. Patients with RA who stop methotrexate abruptly risk accelerated joint erosion. Patients with lupus who stop hydroxychloroquine face increased risk of flare involving kidneys and the central nervous system. The risk is not hypothetical — it is documented in clinical literature across every major autoimmune category.
For pregnant or nursing patients managing autoimmune disease: consult your obstetrician and rheumatologist before making any changes to your medication regimen. Both autoimmune disease activity and standard treatments carry pregnancy-specific risk profiles that require specialist coordination. No peptide discussed in this article has established safety data for use during pregnancy.
The Established Treatment Landscape and Why It Exists
The modern pharmacology of autoimmune disease represents decades of targeted drug development aimed at the specific immune pathways that drive each condition. It is worth understanding what these therapies do, because the complexity is precisely why self-managing this territory with grey-market compounds is not a comparable alternative.
Conventional DMARDs (methotrexate, hydroxychloroquine, sulfasalazine, leflunomide) reduce immune system activity broadly and have been in clinical use for decades. Methotrexate, the anchor DMARD for rheumatoid arthritis, inhibits folate metabolism in rapidly dividing immune cells. It requires regular liver function tests and is teratogenic — but its efficacy and safety profile at appropriate doses under monitoring is well established.
Biologic DMARDs target specific immune proteins: TNF-alpha inhibitors (adalimumab, etanercept), IL-6 inhibitors (tocilizumab), IL-17 inhibitors (secukinumab), and B-cell depleting agents (rituximab). These represent the single largest advance in autoimmune treatment in the past 30 years, achieving remission rates in RA, psoriatic arthritis, and ankylosing spondylitis that prior therapies could not reach. They carry increased infection risk, requiring tuberculosis screening before initiation and regular monitoring throughout.
JAK inhibitors (tofacitinib, baricitinib, upadacitinib) block intracellular signaling downstream of cytokine receptors, interrupting the inflammatory cascade with an oral pill. They have demonstrated efficacy in RA, psoriatic arthritis, and ulcerative colitis, but carry an FDA-required boxed warning for serious infections, malignancy, and cardiovascular events — risks that are documented and monitored, not hidden.
The complexity here is not a failure of medicine to find something simpler. It reflects decades of learning, through controlled trials and post-marketing surveillance, what actually modifies disease course. Peptides may eventually contribute — thymosin alpha-1 is being studied for serious reasons — but the path from "interesting mechanism in a mouse" to "safe adjunct in a patient already on three immunomodulatory drugs" runs through regulatory science, not wellness Instagram.

Evidence-Based Adjuncts That Complement Prescribed Therapy
The good news for patients who want to support their treatment: there are lifestyle and supplement interventions with actual human evidence for reducing autoimmune disease activity that do not carry the risks of grey-market peptides.
Vitamin D: Low vitamin D is consistently associated with higher disease activity in RA, lupus, and MS. Supplementing to normalize serum levels (typically 40-60 ng/mL 25-OH-D, confirmed by bloodwork) is widely recommended by rheumatologists. Dose and form should be confirmed with your physician.
Omega-3 fatty acids: EPA and DHA from fish oil inhibit arachidonic acid-derived prostaglandins and leukotrienes. Meta-analyses in RA show modest but consistent reductions in morning stiffness and tender joint counts at 2-4 grams EPA+DHA daily. This is adjunct support, not disease modification.
Sleep quality: Disrupted sleep elevates IL-6, TNF-alpha, and other pro-inflammatory cytokines. For patients with inflammatory autoimmune disease, poor sleep is not just uncomfortable — it is mechanistically relevant to flare activity. This is an area where behavioral intervention (sleep hygiene, treating comorbid sleep apnea, managing pain that disrupts sleep) can reduce inflammatory burden without touching the immune system pharmacologically.
These adjuncts work alongside prescribed therapy, not instead of it. The [peptides-for-inflammation] overview covers additional research on the general anti-inflammatory potential of specific peptides, and our [peptides-and-medications] guide addresses what is known about peptide interactions with common autoimmune drugs.
Frequently Asked Questions
Are there any peptides FDA-approved for autoimmune disease? No. As of early 2026, no peptide is FDA-approved in the United States for an autoimmune indication. Thymosin alpha-1 is approved in other countries for hepatitis and oncology adjunct use, but not in the U.S. for autoimmune disease.
Can thymosin alpha-1 be prescribed by a doctor in the U.S.? Since the FDA placed Ta1 on the 503A bulk substances list in 2023, licensed compounding pharmacies cannot legally compound it for individual patients without specific exemption. Obtaining it means sourcing it outside the regulated pharmaceutical supply chain.
Does low-dose naltrexone interact with autoimmune medications? LDN at 1.5-4.5 mg is generally considered low-interaction, but it is an opioid antagonist with immune-modulating effects. Any patient on immunosuppressive therapy should discuss LDN with their rheumatologist before trying it. The combination has not been systematically studied in randomized trials.
What about peptides for autoimmune skin conditions like psoriasis or eczema? Barrier-repair peptides in topical cosmetics are distinct from systemically administered immune-modulating compounds. Biologic therapies (IL-17, IL-23, and IL-4/13 inhibitors) are approved for moderate-to-severe psoriasis and atopic dermatitis and represent the current standard of care when topical treatment falls short.
I've heard BPC-157 cures Crohn's disease. Is that true? No. There is no published human clinical trial demonstrating BPC-157 treats Crohn's disease. The claim circulates based on rat colitis studies. Rodent inflammation models are useful research tools, but they do not predict human outcomes reliably enough to justify self-treatment with an unapproved compound — particularly when FDA-approved biologics with demonstrated Crohn's remission data already exist.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion
The research on peptides and autoimmune conditions is real, early-stage, and genuinely interesting — particularly for thymosin alpha-1, which has a substantive human trial record and a plausible mechanism. But "genuinely interesting" and "safe to self-administer instead of your prescribed rheumatology regimen" are not the same conclusion. The FDA approval gap exists because the regulatory process answers questions forums and wellness vendors do not: Does this compound work in a controlled human population? What happens when you give it to someone already on immunosuppressants? What are the long-term risks?
If you are curious about any compound discussed here, the right conversation is with your rheumatologist, neurologist, or gastroenterologist. The [are-peptides-safe] overview covers how to evaluate peptide evidence before that conversation. Some physicians do incorporate thymosin alpha-1 or LDN into integrative protocols alongside standard-of-care therapy, with monitoring. That is a very different proposition from a vial of unknown provenance ordered from an overseas website.
Your immune system is already working against you in a precise, mechanistically specific way. The treatments designed to address that precision are worth taking seriously.
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any changes to your medication regimen or starting any new supplement or compound. Do not stop or modify prescribed autoimmune therapy without rheumatologist supervision. Discontinuing a DMARD or biologic without specialist guidance can trigger disease flare and permanent organ damage.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
