If you are researching CJC-1295 and ipamorelin, you have probably read that stacking these two peptides is the "gold standard" for growth hormone optimization. That claim is circulating in forums, fitness podcasts, and grey-market vendor copy with a confidence the published literature does not support. So before this article explains the pharmacology, here is the honest answer upfront.
Neither CJC-1295 nor ipamorelin is FDA-approved for human use. No published randomized controlled trial has tested the specific combination in humans. The biological rationale for stacking them is real, but the clinical evidence that the stack produces meaningful outcomes in healthy adults is essentially absent.
That context does not make the pharmacology uninteresting. It makes it more important to understand clearly.
Summary: Both Peptides at a Glance
| Property | CJC-1295 | Ipamorelin |
|---|---|---|
| Mechanism | GHRH analog (hypothalamus-side) | GHS-R1a agonist (pituitary-side) |
| Target receptor | GHRH receptor on pituitary somatotrophs | Ghrelin receptor (GHS-R1a) |
| FDA approval | NOT approved | NOT approved |
| Half-life (no DAC) | ~30 minutes (similar to native GHRH) | ~2 hours |
| Half-life (with DAC) | 5.8-8.1 days | N/A |
| Cortisol/ACTH effect | Minimal at therapeutic doses | Minimal (key selectivity advantage) |
| Prolactin effect | Minimal | Minimal |
| WADA status | Prohibited (S2.2.4) | Prohibited (S2.2.4) |
| Human RCT evidence | 1 pharmacokinetic study (n=64) | Primarily animal and in vitro data |
| Evidence for the stack | No published human RCTs | No published human RCTs |
Best for: Understanding the mechanistic science and asking informed questions of a licensed physician. Not for: Anyone expecting peer-reviewed proof that this stack builds muscle or burns fat in healthy adults; athletes in WADA-tested sport (career-ending risk).
What Is CJC-1295?
CJC-1295 is a synthetic 30-amino acid analog of growth hormone-releasing hormone (GHRH), the peptide produced in the hypothalamus that signals the pituitary to release growth hormone. Native GHRH has a plasma half-life of roughly two to seven minutes because two enzymes — dipeptidyl peptidase IV (DPP-IV) and neutral endopeptidase — cleave it rapidly. CJC-1295 was engineered to resist that cleavage, extending its active window substantially.
The compound comes in two variants that matter clinically. CJC-1295 without Drug Affinity Complex (no-DAC) behaves somewhat like an extended native GHRH: it is active for several hours before clearance. CJC-1295 with Drug Affinity Complex (DAC) covalently binds to serum albumin after injection, creating a depot effect. The human pharmacokinetic data from Teichman et al. (PMID 16352683) — the only published randomized double-blind trial in humans — found that a single injection of CJC-1295 with DAC produced a half-life of 5.8 to 8.1 days, with mean plasma GH concentrations rising 2- to 10-fold for six or more days and IGF-1 remaining elevated 1.5- to 3-fold for 9 to 11 days.
The pharmacokinetic implication of the DAC version is significant and often glossed over. A compound that elevates GH continuously for nearly two weeks does not produce the pulsatile GH release pattern the body uses physiologically. Pulsatile release is thought to be important for maintaining GH receptor sensitivity and avoiding tachyphylaxis. Whether sustained GH elevation carries different risks than pulsatile stimulation is not established in the published literature — the Teichman study was powered to measure pharmacokinetics over a short window, not to detect long-term endocrine consequences.
What the study did not measure: muscle mass, strength, body composition, or any outcome relevant to fitness or performance. It was a dose-escalation pharmacokinetics study, and interpreting its results as evidence that CJC-1295 improves body composition requires a logical leap the data does not support.
The FDA has placed CJC-1295 on its list of bulk drug substances that present "demonstrable difficulties for compounding" due to safety concerns, effectively restricting its use in compounding pharmacies. CJC-1295 is NOT FDA-approved as a drug or dietary supplement.
Actionable takeaway: If you encounter CJC-1295 marketed as a supplement or sold without a prescription, that product is not legally sold for human use in the United States, regardless of how the label describes it.
What Is Ipamorelin?
Ipamorelin is a synthetic pentapeptide that acts as a selective agonist at the ghrelin receptor, also called the growth hormone secretagogue receptor 1a (GHS-R1a). Its action is on the pituitary side of the GH axis, where it stimulates somatotroph cells to release GH in discrete pulses. The receptor it binds is different from the GHRH receptor that CJC-1295 targets — a distinction that forms the mechanistic argument for stacking the two compounds.
The pharmacological characteristic that distinguishes ipamorelin from older GHRPs like GHRP-2 and GHRP-6 is its hormonal selectivity. Raun et al. (PMID 9849822) demonstrated that in conscious swine, ipamorelin produced robust GH release comparable to GHRP-6, but unlike GHRP-2 and GHRP-6, it did not produce significant elevations in ACTH or cortisol even at doses 200-fold above the effective GH-stimulating threshold. The authors concluded ipamorelin was "the first GHRP-receptor agonist with a selectivity for GH release similar to that displayed by GHRH." This selectivity is the reason ipamorelin displaced GHRP-2 and GHRP-6 in clinical research and in grey-market use: fewer off-target hormonal effects in the experimental data.
That finding deserves a skepticism check. It comes from animal data published in 1998. Human cortisol and ACTH response data for ipamorelin is not robust. Extrapolating from porcine pharmacology to human endocrinology is a methodological gap the marketing material reliably omits. No large-scale human randomized trial has confirmed that ipamorelin's cortisol-sparing profile holds across populations, doses, and protocols that people actually use.
Ipamorelin has an approximate plasma half-life of two hours in animal studies, meaning it produces a defined GH pulse rather than the prolonged elevation seen with CJC-1295 with DAC. This pulsatile characteristic is often cited as more physiologically normal, though "more physiological" is not the same as "safe" or "effective for the claimed use" in human clinical terms.
Ipamorelin is NOT FDA-approved for any indication. It has not cleared Phase III clinical trials for any human condition.
Why They Are Often Stacked: The GHRH + GHRP Synergy Theory
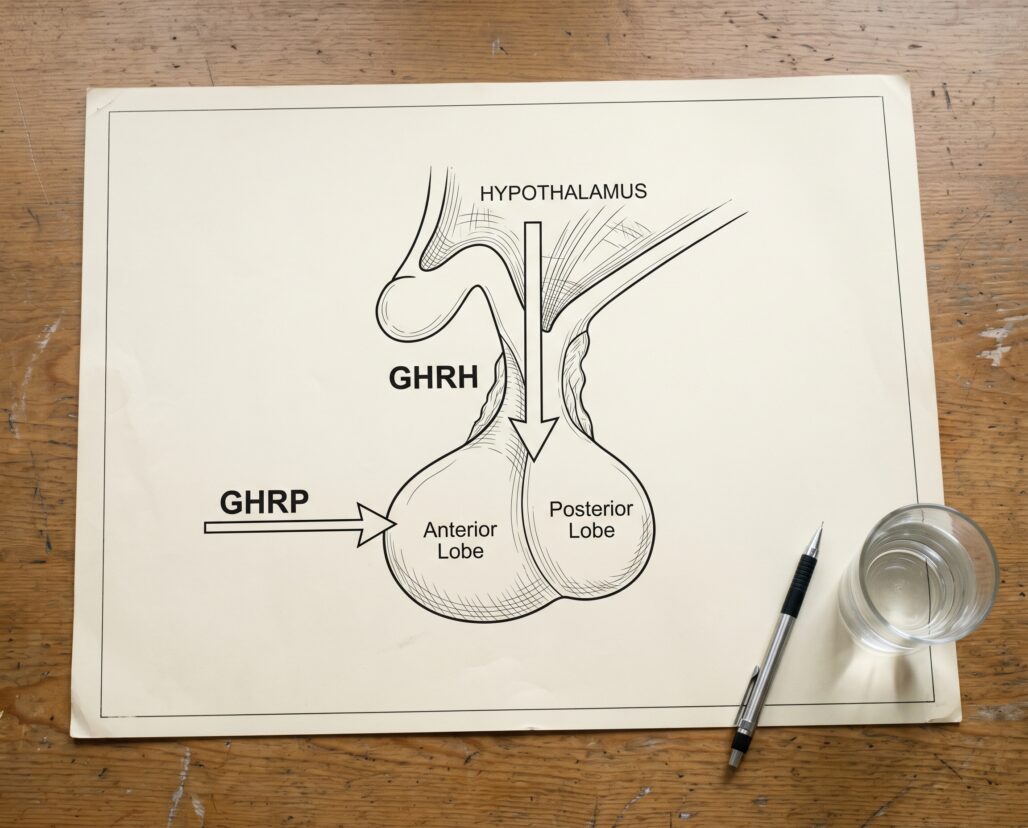
The rationale for combining CJC-1295 and ipamorelin is grounded in genuine biology. The GH axis has two primary stimulatory inputs operating through distinct receptor systems:
- GHRH (hypothalamus) binds the GHRH receptor on pituitary somatotroph cells, increasing cyclic AMP (cAMP) and activating protein kinase A, which raises intracellular calcium and drives GH vesicle exocytosis.
- GHS-R1a agonists (GHRPs) act on the ghrelin receptor on those same somatotroph cells through a different intracellular pathway, also raising intracellular calcium. They additionally act at the hypothalamus to suppress somatostatin — the natural "off switch" for GH release.
When both receptor systems are activated simultaneously, the GH response is larger than the sum of either stimulus alone. This is the synergy effect that stacking proponents cite. The underlying receptor physiology is real and well-described in the pharmacological literature. GHRH analogs and GHRPs do work through distinct, complementary pathways.
The problem is not the biology. The problem is the evidence gap between "these two mechanisms are complementary" and "stacking these two specific compounds in humans produces clinically meaningful outcomes." No published randomized controlled trial has administered CJC-1295 and ipamorelin together to human participants and measured body composition, strength, or any patient-relevant endpoint. The synergy argument rests on mechanistic theory and animal data — not on human clinical trial evidence.
A useful analogy: knowing that braking force and steering act through different mechanical systems does not tell you how a specific car will perform on a specific road. The mechanism is real; the performance claim requires testing.
Actionable takeaway: The biological rationale for stacking a GHRH analog with a GHRP is not pseudoscience. The claim that stacking them works for any specific human outcome is not supported by published clinical evidence.
What Human Evidence Exists for Each Compound Separately?
For CJC-1295, the human evidence consists of the Teichman et al. 2006 study (PMID 16352683): a randomized double-blind dose-response trial in 64 healthy adults confirming sustained GH and IGF-1 elevation with acceptable short-term safety. It measured no muscle mass, strength, or performance outcomes. That is the full scope of published controlled human evidence for CJC-1295.
For ipamorelin, published human controlled trial data is thinner still. The compound's selectivity advantage over GHRP-2 and GHRP-6 was established in animal models (Raun et al., PMID 9849822). Ipamorelin did not advance to Phase III trials for any human indication.
For GH secretagogues as a class, a systematic review of 27 randomized controlled trials found that GH administration itself produced a modest 2.1 kg increase in lean body mass but that "strength and exercise capacity did not seem to improve" (PMID 18347346). If direct GH administration does not reliably convert to strength gains, the case for upstream secretagogues requires even more evidence than currently exists.
Oral secretagogues like MK-677 have more human data — including reversal of diet-induced nitrogen wasting (PMID 9467534) — but those findings do not transfer to injectable peptides with different pharmacokinetics.
What Evidence Exists for the Stack Specifically?
None from peer-reviewed randomized controlled trials in humans. This is not a minor caveat — it is the defining limitation for anyone weighing the risk-benefit calculus of using this combination.
Grey-market forums and vendor sites cite anecdotal reports and mechanistic theory. Some compounding pharmacy literature discusses the combination, but compounded drug protocols are not subject to the same clinical trial requirements as FDA-approved drugs, meaning the "clinical experience" cited in those contexts is not equivalent to controlled evidence.
The absence of human RCT data for the stack means there is no controlled information about optimal dosing, frequency, long-term safety, or actual efficacy for any outcome in healthy adults. People using this combination are, in any honest framing, conducting an uncontrolled self-experiment with compounds that have not been tested at the doses and frequencies being used.
Actionable takeaway: Before accepting any claim about what the CJC-1295 + ipamorelin stack "does," ask: "Does a published human RCT support this claim for this specific combination?" The answer is currently no.
Regulatory Status: What the Rules Actually Say
FDA status: Neither CJC-1295 nor ipamorelin is approved by the U.S. Food and Drug Administration as a drug or dietary supplement. The FDA's position on CJC-1295 in compounding contexts explicitly cites safety concerns, and both compounds are not legally available for human use through legitimate commercial channels without an active investigational new drug (IND) application. Products sold on research-chemical websites with "for research use only" disclaimers are not a legal workaround — they are the same compounds with different labeling.
WADA prohibition: Both CJC-1295 and ipamorelin are explicitly named on the World Anti-Doping Agency Prohibited List. CJC-1295 appears under S2.2.4 as a GHRH analog. Ipamorelin appears under S2.2.4 as a growth hormone secretagogue. Both are classified as non-Specified Substances, which carries the strictest sanction tier — with limited room for reduced punishment in the event of a positive test. Any athlete competing under a WADA signatory federation who uses either compound faces the risk of a ban.
Pregnancy and nursing: Both compounds carry complete uncertainty regarding fetal and infant safety. No safety data exists for use during pregnancy or breastfeeding. Blanket avoidance applies.
Side-by-Side Comparison Table
| Property | CJC-1295 (no DAC) | CJC-1295 (with DAC) | Ipamorelin |
|---|---|---|---|
| Classification | GHRH analog | GHRH analog + albumin-binder | GHRP / GHS-R1a agonist |
| Receptor | GHRH receptor | GHRH receptor | Ghrelin receptor (GHS-R1a) |
| Half-life | ~30 min | 5.8-8.1 days | ~2 hours |
| GH release pattern | Pulsatile | Sustained elevation | Pulsatile |
| Cortisol/ACTH impact | Low | Low | Very low (vs GHRP-2/6) |
| Human RCT data | Yes (pharmacokinetics only) | Yes (pharmacokinetics only) | Minimal |
| Muscle/performance RCT | None | None | None |
| FDA approved | No | No | No |
| WADA prohibited | Yes (S2.2.4) | Yes (S2.2.4) | Yes (S2.2.4) |

Frequently Asked Questions
Is CJC-1295 with DAC better than without DAC for stacking with ipamorelin? The no-DAC version produces shorter, more pulsatile GH release. Some researchers prefer it on the grounds that sustained GH elevation from the DAC version may blunt receptor sensitivity over time. No human trial has compared the two variants in combination with ipamorelin, so this is pharmacological reasoning rather than clinical guidance.
Does the stack cause more side effects than either compound alone? Unknown. No human trial has examined combined adverse effects. Known individual side effects of GHRH analogs and GHRPs include injection-site reactions, water retention, extremity tingling, and headache. Whether these are additive when the peptides are combined has not been studied in a controlled setting.
How does ipamorelin compare to GHRP-2 or GHRP-6 for stacking purposes? See the companion article on GHRP-2 vs. GHRP-6 for a full breakdown. The short answer: ipamorelin's selective hormonal profile — GH release without proportional ACTH and cortisol elevation — is the pharmacological basis for preferring it. Whether this translates to better human outcomes is untested.
Can I legally get CJC-1295 or ipamorelin prescribed? Neither compound has an FDA-approved indication. Some compounding pharmacies have prepared them under prescriber supervision, but FDA regulatory actions have increasingly restricted that pathway. Consult a licensed physician for current legal options.
Does the stack actually build muscle? No published randomized controlled trial tests the CJC-1295 + ipamorelin combination for hypertrophy or strength in humans. Forum reports are not controlled evidence.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion
CJC-1295 and ipamorelin occupy different positions in the GH axis — one acting at the hypothalamus-side GHRH receptor to amplify GH pulse amplitude, the other acting at the pituitary-side ghrelin receptor to trigger additional GH release and suppress somatostatin. The mechanistic argument for combining them is biologically coherent. The biological coherence of a theory does not constitute clinical evidence that the theory produces the outcomes people use these compounds for.
For CJC-1295, a single human pharmacokinetic study confirms that the compound raises GH and IGF-1 in healthy adults for extended periods. For ipamorelin, animal data establishes its selectivity advantage over older GHRPs. For the stack, there is no published human randomized controlled trial. For both compounds, the regulatory position is clear: neither is FDA-approved, both are WADA-prohibited, and both face restrictions on legitimate availability in the United States.
For deeper pharmacology, the neighbor articles on CJC-1295 explained and ipamorelin explained cover each compound's mechanism in detail. For broader context on how these compounds fit into performance use, see peptides for bodybuilding. If you are an athlete in a tested sport, the WADA prohibition is unambiguous and the career consequences of a positive test are disproportionate to any unproven benefit.
Actionable takeaway: The synergy rationale is the strongest argument for this stack. It is not a substitute for clinical trial data — and that data does not yet exist.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
