There is a version of the PCOS conversation that has not aged well. A decade ago, most endocrinologists handed patients a metformin prescription and told them to lose weight. That advice was not wrong, exactly, but it skipped over how hard weight loss is when insulin resistance is working against you and how many patients cycle through metformin without meaningful metabolic improvement. GLP-1 receptor agonists have substantially changed how endocrinologists think about metabolic intervention in this condition. They are now appearing in PCOS management discussions at a frequency that the research has not quite caught up with. No GLP-1 drug has an FDA-approved indication for PCOS. The 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome positions these agents as a consideration for a narrow subset of patients after first-line options have been tried (PMID 37580314). Understanding exactly where the evidence supports their use, and where it runs out, is the starting point for any useful conversation with an endocrinologist. This article walks through the underlying biology, the trial data, how inositol fits in, and what a realistic clinical pathway looks like.
Summary / Quick Answer
No peptide or GLP-1 receptor agonist has FDA approval specifically for PCOS. Metformin remains the first-line pharmacological treatment per the 2023 international guideline. GLP-1 receptor agonists are used off-label, primarily for weight management in patients with PCOS and obesity, when lifestyle modification and first-line therapy have been insufficient. Inositol has a separate evidence base as a supplement with moderate-quality trial data supporting improvements in insulin resistance and ovulation rates.
- Who this is for: Women with PCOS dealing with insulin resistance, obesity, and difficulty with menstrual regularity who have not achieved goals on lifestyle changes and metformin alone
- Not a starting point: GLP-1 agents are not first-line for PCOS and require specialist supervision — they are off-label, prescription-only medications
- Fertility note: If you are trying to conceive, GLP-1 receptor agonists must be discontinued at least two months before attempting conception; discuss timing explicitly with your reproductive endocrinologist
- Compounded GLP-1s: The FDA has issued explicit caution about compounded versions of semaglutide and tirzepatide — quality, sterility, and dosing accuracy are not guaranteed; these are not equivalent to approved products
What PCOS Actually Is: Insulin Resistance at the Center
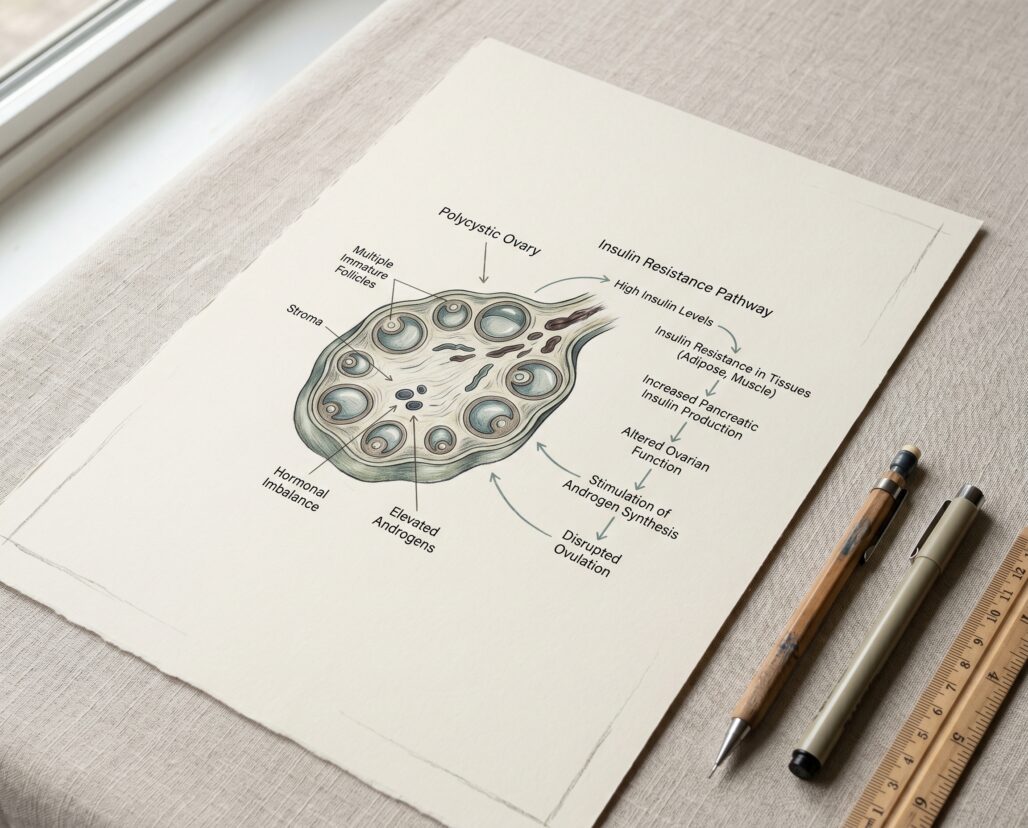
Polycystic ovary syndrome affects an estimated 8 to 13 percent of women of reproductive age, making it the most common endocrine disorder in that population. The name is misleading. Cysts on the ovaries are neither required for diagnosis nor the primary driver of the condition's most disruptive effects. The Rotterdam Criteria, which most clinicians use, require two of three findings: irregular or absent ovulation, clinical or biochemical signs of hyperandrogenism (excess androgen hormones), and polycystic ovarian morphology on ultrasound.
What ties those three together is insulin resistance, which appears in roughly 70 to 80 percent of women with PCOS regardless of body weight. Excess insulin signals the ovarian theca cells to produce more androgens, particularly testosterone. Elevated androgens disrupt follicle maturation and ovulation, leading to the irregular cycles that are often a person's first visible sign that something is off. Chronically elevated insulin also suppresses sex hormone-binding globulin (SHBG), which normally acts as a buffer by binding free testosterone. Lower SHBG means more free testosterone in circulation.
The downstream consequences are not limited to reproductive function. Insulin resistance raises long-term cardiovascular risk, is a precursor to type 2 diabetes in a significant proportion of affected women, and contributes to the dyslipidemia frequently seen in PCOS patients. This is why interventions that address insulin sensitivity are central to PCOS management, not peripheral to it.
Metformin: Still the First-Line Reference Point
Before turning to GLP-1 receptor agonists, it is worth being explicit about where the clinical consensus stands on first-line pharmacotherapy.
Metformin is a biguanide, not a peptide. It works primarily by reducing hepatic glucose output and improving peripheral insulin sensitivity. It has been used in PCOS for decades and has accumulated a large evidence base. The 2023 International Evidence-Based Guideline for Assessment and Management of Polycystic Ovary Syndrome, published simultaneously in the Journal of Clinical Endocrinology and Metabolism, European Journal of Endocrinology, and Fertility and Sterility (PMID 37580314), recommends metformin alongside lifestyle modification as the primary pharmacological approach for metabolic management in PCOS. It is not off-label in this context. It has a long safety record, is inexpensive, and is generally well-tolerated at titrated doses.
Why does this matter? Because GLP-1 receptor agonists are sometimes discussed as if they represent a direct upgrade or replacement for metformin. The current evidence does not support that framing. The two agents have different mechanisms, different approval statuses in PCOS specifically, and different risk profiles, particularly around pregnancy. Any consideration of GLP-1 therapy in PCOS should happen against the backdrop of what has already been tried with first-line approaches.
GLP-1 Receptor Agonists for PCOS: Off-Label, But With Growing Trial Data
GLP-1 receptor agonists — including liraglutide (Victoza, Saxenda), semaglutide (Ozempic, Wegovy), and exenatide (Byetta, Bydureon) — are synthetic peptide analogues of glucagon-like peptide-1, a gut hormone that stimulates insulin secretion in a glucose-dependent manner, slows gastric emptying, and reduces appetite through central nervous system signaling. None of them carry an FDA-approved indication for PCOS. They are prescribed off-label in this context, and any use requires physician oversight.
The 2023 international PCOS guideline (PMID 37580314) positions GLP-1 receptor agonists as a consideration for weight management in women with PCOS and obesity when lifestyle intervention and first-line pharmacotherapy have not achieved adequate results. That is a specific, conditional framing. It is not a broad endorsement.
What the meta-analysis data shows:
A 2024 meta-analysis of randomized controlled trials examined GLP-1 agonist use in women with PCOS and obesity (PMID 39178623). Across four RCTs involving 176 participants — predominantly using liraglutide, with some semaglutide data — GLP-1 agonists produced significant reductions in waist circumference (-5.16 cm), BMI (-2.42 kg/m squared), and triglycerides. Total testosterone fell by 1.33 ng/dL. A note of caution: improvements in HOMA-IR, the standard measure of insulin resistance, did not reach statistical significance in this pooled analysis (p = 0.35). That does not mean GLP-1 agents are ineffective for insulin resistance in PCOS; it means the trials were small and the pooled estimates are wide.
A larger 2023 systematic review and meta-analysis analyzed 11 RCTs comprising 840 patients with PCOS (PMID 37940910). GLP-1 receptor agonists improved natural pregnancy rates (relative risk 1.72, 95% CI 1.22 to 2.43), menstrual regularity, SHBG levels, BMI, and waist circumference versus control groups. Notably, the review found that GLP-1 monotherapy was not consistently superior to metformin for free testosterone and DHEAS specifically — a finding worth flagging for anyone assuming these agents outperform the first-line option across all PCOS markers.
A 2024 scoping review focused specifically on weight-loss outcomes (PMID 39262529) found that liraglutide and exenatide uniformly reduced weight, BMI, and total fat percentage across the reviewed studies, with positive effects on menstrual regulation and natural pregnancy rates. The authors were appropriately cautious: long-term effects remain undetermined, and further research is warranted before these agents become standard of care in PCOS.
A 2025 network meta-analysis comparing pharmacological interventions in PCOS (PMID 39955537) found that adding GLP-1 receptor agonists to standard therapy significantly reduced body weight, BMI, waist circumference, HOMA-IR, and fasting blood glucose versus standard therapy alone — providing some of the more favorable metabolic data yet, though the authors noted the trials underlying these estimates vary in duration and population.
The pregnancy timing issue:
If you have PCOS and are actively trying to conceive, GLP-1 receptor agonists are not appropriate for concurrent use. The FDA labels for all approved GLP-1 agents recommend discontinuation before attempting pregnancy — at minimum two months prior to conception attempt — due to insufficient safety data in human pregnancy and adverse findings in animal studies. For PCOS patients, this timing consideration is particularly important to discuss explicitly with a reproductive endocrinologist, because improving ovulation through weight loss may inadvertently increase conception probability during treatment.
Side effects:
Nausea, vomiting, and abdominal discomfort are the most common. In the 2024 meta-analysis, 49 of 112 patients with adverse event data reported gastrointestinal side effects. Most are dose-dependent and tend to diminish with gradual titration. Pancreatitis is a rare but serious concern documented across the GLP-1 drug class.
Inositol: A Different Evidence Stream
Inositol sits in a different category from GLP-1 receptor agonists. It is a naturally occurring polyol found in food and synthesized in the body. Two forms are relevant to PCOS: myo-inositol (MI) and d-chiro-inositol (DCI). Both function as second messengers in insulin signaling pathways, and both have been tested as supplements, not prescription medications, in PCOS.
A 2026 umbrella review synthesizing 13 meta-analyses from randomized controlled trials (PMID 41757236) provides the most comprehensive summary of the evidence to date. Findings included:
- LH reduced by 3.43 IU/L
- Free testosterone decreased by 0.02 nmol/L
- SHBG increased by 36.72 nmol/L
- HOMA-IR decreased by 1.14
- Fasting insulin reduced by 23.40 pmol/L
- Ovulation rate improved (risk ratio 2.75)
- Live birth rate improved (risk ratio 2.29)
The evidence quality assessment is important context. The authors found that most findings were supported by very low to moderate quality evidence — meaning residual confounding, small trial sizes, and heterogeneity in populations and dosing are real concerns. The conclusion is not that inositol does not work. It is that the effect estimates carry uncertainty.
On dosing and form: myo-inositol monotherapy showed superior metabolic outcomes compared to d-chiro-inositol alone in this umbrella review. A combined ratio of 40:1 myo-inositol to d-chiro-inositol has been widely studied and is the basis for most commercial inositol supplements targeting PCOS. Doses used across trials typically range from 2g to 4g of myo-inositol daily, often with folic acid co-supplementation.
Where inositol fits relative to GLP-1 agents:
Inositol and GLP-1 receptor agonists are not competing alternatives. They operate through different mechanisms, carry different risk profiles, and are regulated differently. Inositol is an over-the-counter supplement; GLP-1 agents are prescription medications. Inositol is generally considered safe in pregnancy and is sometimes used to support fertility outcomes; GLP-1 agents must be stopped before conception. Inositol's effect sizes are modest by most estimates; GLP-1 agents produce substantially larger weight reductions in the short term. A patient with severe obesity and marked insulin resistance will not get the same metabolic leverage from inositol that liraglutide or semaglutide can provide. A patient with mild insulin resistance who is trying to conceive may be better served starting with inositol while pursuing lifestyle modification.
Where Peptides Actually Fit in PCOS Management
GLP-1 receptor agonists are not a PCOS treatment in the sense that they target the underlying condition. They are weight management tools that, in women with PCOS and significant obesity, produce downstream improvements in the metabolic and hormonal features that drive PCOS symptoms. The weight loss is the mechanism — not a direct correction of ovarian function or androgen production.
For a patient who has tried metformin at therapeutic doses, implemented a structured lifestyle program, and still has obesity-driven PCOS symptoms, GLP-1 therapy is a reasonable next conversation with an endocrinologist. It is not appropriate as a first step, not appropriate during attempted conception, and not appropriate from a compounding pharmacy where quality and dosing accuracy are not guaranteed. The FDA has issued explicit caution about compounded semaglutide and tirzepatide — including concerns about incorrect dosing, contamination, and unapproved salt forms.
Neither GLP-1 agents nor inositol replace the foundational work: a dietary pattern that moderates glycemic load, consistent resistance exercise, and regular metabolic monitoring.
Discussing GLP-1s With Your Endocrinologist
If you are considering raising GLP-1 receptor agonists as a conversation topic with an endocrinologist or reproductive endocrinologist, the following questions are likely to be productive:
"Have I met the criteria where off-label GLP-1 use would be appropriate for me?" The 2023 international guideline suggests these agents are relevant when lifestyle intervention and first-line pharmacotherapy have been insufficient for weight management in a patient with obesity. If you have not yet tried metformin at therapeutic doses or implemented a structured lifestyle intervention, that step comes first.
"What does my HOMA-IR look like, and how do we define success?" HOMA-IR is a fasting insulin and glucose-derived estimate of insulin resistance. Having a baseline value and a target helps evaluate whether any intervention is doing what it is supposed to do.
"What is the plan around contraception and fertility timing?" For PCOS patients, where irregular cycles can mask ovulation, the interaction between improved ovulation on GLP-1 therapy and the need to discontinue before conception requires explicit planning, not an afterthought.
"Is my prescriber comfortable with off-label management of PCOS, or should I see a specialist?" General practitioners vary considerably in their familiarity with the PCOS guideline literature. An endocrinologist or reproductive endocrinologist with specific PCOS experience is the appropriate resource for nuanced pharmacological management.
Frequently Asked Questions
Can I take inositol and metformin together?
Some trials have combined them, and a 2025 study found combination inositol and metformin produced favorable metabolic outcomes, particularly for certain PCOS phenotypes. There is no well-documented pharmacological conflict between the two, but your prescribing physician should be aware of both if you are taking metformin and adding an inositol supplement.
Does weight loss "cure" PCOS?
No. PCOS is a chronic condition. Significant weight loss can dramatically reduce the severity of symptoms — improving ovulation, reducing androgen levels, and lowering insulin resistance — but the underlying predisposition remains. Many women find that symptoms return if weight is regained.
Is semaglutide being studied specifically in PCOS?
Yes. A 2026 pilot prospective study (PMID 41421448) examined semaglutide with metformin in PCOS patients with obesity, reporting significant weight reduction and improved fertility outcomes. These are early-stage findings from small studies, not evidence that changes prescribing guidelines. More rigorous trials are needed.
Are GLP-1 receptor agonists safe during pregnancy?
No. Current labeling for all approved GLP-1 receptor agonists recommends discontinuation before attempting conception. A 2026 systematic review found that early-pregnancy exposure is not consistently associated with increased risk, but the evidence base is insufficient to establish safety, and current clinical guidance is to stop these agents before trying to conceive (PMID 41885132).
Conclusion
GLP-1 receptor agonists have a legitimate and growing role in PCOS management for a specific subset of patients, but that role is narrower and more conditional than the current level of clinical discussion might suggest. No peptide-based drug is FDA-approved for PCOS. Metformin and lifestyle modification remain the first-line approach per the 2023 international guideline. GLP-1 agents enter the picture as off-label tools for weight management when first-line options have not been sufficient — and they require specialist supervision, reliable contraception during use, and discontinuation well before any conception attempt.
Inositol occupies a different niche: a supplement with moderate-quality evidence for modest improvements in insulin sensitivity and ovulation rates, relevant especially for patients who are trying to conceive or who are not candidates for prescription weight management therapy.
If you have PCOS and are trying to understand whether any of these options apply to your situation, the most useful first step is a conversation with an endocrinologist who can review your metabolic labs, reproductive goals, and full medication history. For further context on how GLP-1 agents work mechanistically, see our complete semaglutide guide and the broader peptides-for-weight-loss review.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
