If you search "peptides for perimenopause" right now, the results split into two camps that could not be further apart in terms of evidence: on one side, FDA-approved injectable GLP-1 receptor agonists with large randomized trial data on weight and metabolic outcomes; on the other, a broad category of unregulated peptide products making claims about "hormonal rebalancing" that no supplement has ever demonstrated. Somewhere in the middle sits collagen peptide supplementation, which has a modest but real randomized trial record — just not for the symptoms most women are actually hoping to address. Sorting out which category applies to which perimenopausal concern, and where hormone replacement therapy remains the evidence-backed standard, requires looking at the physiology first and the marketing second.
Summary / Quick Answer
The honest short answer: perimenopause involves several distinct physiological shifts that do not all respond to the same interventions. Collagen peptides have RCT evidence for skin and bone markers but not for hot flashes or vasomotor symptoms. GLP-1 receptor agonists are used off-label for perimenopausal weight gain and carry strong evidence for weight reduction but no perimenopause-specific indication. For vasomotor symptoms, the North American Menopause Society identifies hormone therapy as the most effective treatment for eligible women — no peptide category has evidence comparable to HRT at this level.
Best candidates for peptide use in this life stage:
- Women managing body composition changes who are working with an endocrinologist on pharmacologic weight management (GLP-1s as off-label option)
- Women focused on skin elasticity, dermal collagen density, or connective tissue as a complement to an existing routine (oral collagen peptides)
- Women at high fracture risk who have been referred to an endocrinologist and have already exhausted first-line options like bisphosphonates (peptide-based teriparatide, covered separately in our teriparatide guide)
Where peptides are not the right conversation:
- Vasomotor symptoms (hot flashes, night sweats): HRT per NAMS 2022 guidance, discussed below
- Genitourinary changes: local or systemic estrogen therapy, not supplements
- Compounded "bioidentical hormones" sold as peptides: not the same as evidence-based HRT; the evidence base is weaker and regulatory oversight is limited
Decision shortcut: If you are in the menopausal transition and your primary concerns are hot flashes, sleep disruption from night sweats, or mood changes tied to hormonal flux, that conversation starts with a gynecologist or menopause specialist — not a supplement stack.
What Perimenopause Actually Is (And Why the Timing Matters)
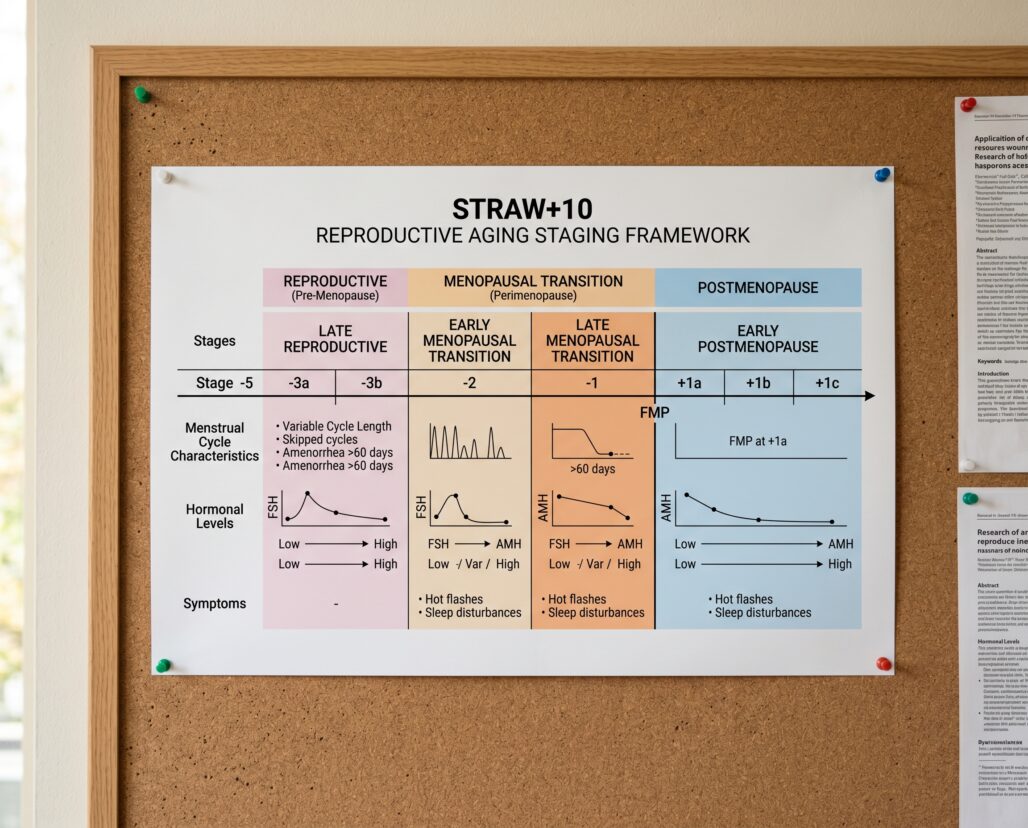
"Perimenopause" is used loosely in popular culture to mean almost any hormonal flux before menopause, which creates real confusion about what is actually happening physiologically at any given point. The STRAW+10 framework — published in 2012 by Harlow and colleagues across four journals including the Journal of Clinical Endocrinology and Metabolism (PMID 22344196) — provides the clinical standard for staging the reproductive aging process.
Under STRAW+10, the perimenopause period spans two distinct stages. The early menopausal transition (Stage -2) is defined by persistent irregularity in menstrual cycle length, specifically a change of seven or more days from a woman's normal cycle. Follicle-stimulating hormone (FSH) begins rising but remains highly variable during this stage — a fact that has clinical implications for anyone using a single FSH test to "confirm" perimenopause. A single elevated FSH reading means little; the pattern over time matters. The late menopausal transition (Stage -1) involves amenorrhea intervals of 60 or more consecutive days and marks the period closest to the final menstrual period (FMP). The STRAW+10 framework distinguishes this from early postmenopause, which begins after 12 consecutive months of amenorrhea.
This staging matters because Stage -2 physiology differs meaningfully from Stage -1. High FSH variability in early transition means estrogen can still be near normal — which makes the "estrogen deficiency" framing that dominates supplement marketing premature. By late transition, the consequences for bone and body composition become measurable. Weight gain and hot flashes, the two symptoms most often attributed to perimenopause, have different etiologies and respond to different interventions.
The Weight Gain Pattern: Visceral, Central, and Harder Than Before
Most women who notice weight gain during perimenopause are not simply eating more or moving less. The distribution of fat shifts even when total caloric intake stays the same. Estrogen's role in regulating adipose tissue depot selection — specifically its tendency to promote peripheral (subcutaneous) fat storage over visceral accumulation — weakens as estrogen levels decline. The result is a shift toward central adiposity: abdominal fat that sits deeper around organs and carries greater metabolic consequence than subcutaneous fat of equivalent volume.
A 2026 longitudinal cohort study in Climacteric tracking 841 Chinese women over two decades found metabolic syndrome prevalence rising from 15% in the reproductive stage to 43.9% in late postmenopause (PMID 41504257), driven primarily by abdominal fat accumulation. The visceral redistribution pattern is not population-specific — it is a documented physiological hallmark of the transition, not a lifestyle failure.
The practical consequence: standard dietary and exercise approaches that worked before perimenopause may produce less visible results, which is where GLP-1 receptor agonists enter the conversation.
GLP-1 Receptor Agonists for Perimenopausal Weight Gain: Off-Label, But With Real Evidence
GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) are not approved for any perimenopause-specific indication. That needs to be clear at the outset. Their FDA approvals cover type 2 diabetes management (multiple agents) and chronic weight management in adults with obesity or overweight plus at least one weight-related comorbidity (semaglutide 2.4 mg as Wegovy, liraglutide 3 mg as Saxenda, tirzepatide as Zepbound). A woman in perimenopause who meets those criteria might legitimately qualify under the approved indication — but the indication is weight or metabolic, not hormonal transition.
What the literature says about this population specifically is limited. A 2025 review by Mikdachi and Dunsmoor-Su in Current Opinion in Obstetrics and Gynecology (PMID 39970049) found that GLP-1 receptor agonists are "consistently the most effective pharmacologic option for weight loss" in peri- and postmenopausal women but noted "a paucity of data about this specific population and how they respond to these medications." The large STEP and SURMOUNT trials that established efficacy for semaglutide and tirzepatide included substantial numbers of women, but were not powered or stratified to detect menopausal status as a modifier. The absence of that subgroup analysis is a genuine evidence gap — not evidence of absence of effect.
What is known from general weight-loss research is that GLP-1 agonists reduce visceral fat disproportionately relative to subcutaneous fat — the depot that shifts adversely during menopausal transition. That mechanistic alignment is plausible, but "plausible" is not the same as "demonstrated in a perimenopause-specific RCT."
Two safety points matter here. First, anyone in perimenopause who has not yet reached 12 months of amenorrhea remains potentially fertile. GLP-1 agonists should be discontinued before a planned pregnancy; contraception is necessary if pregnancy is possible. Second, off-label prescribing for perimenopausal weight management requires a physician experienced with both metabolic pharmacology and the menopausal transition — oversight that matters for dosing, side effect monitoring, and confirming that the standard indication criteria are actually met.
Bone Density at Perimenopause: The Window Most Women Miss
Bone loss during the menopausal transition does not begin after menopause — it begins before it. This is one of the most clinically important and least understood aspects of the perimenopause period.
The Study of Women's Health Across the Nation (SWAN) data published by Greendale and colleagues in Journal of Bone and Mineral Research (PMID 21976317) quantified this precisely. In a multiethnic cohort, bone mineral density (BMD) loss began approximately 1 year before the final menstrual period and was most rapid in the 3-year window bracketing the FMP (1 year before through 2 years after). The researchers termed this the "transmenopause" period. Cumulative losses over 10 years were 10.6% at the lumbar spine and 9.1% at the femoral neck — and 7.38% of lumbar spine loss and 5.8% of femoral neck loss occurred within that concentrated transmenopause window alone.
A 2018 review by Karlamangla, Burnett-Bowie, and Crandall in Obstetrics and Gynecology Clinics of North America (PMID 30401551) further characterized this as a structural problem, not just a density one: changes in bone macrostructure and microarchitecture accompany the BMD decline, and markers of bone resorption rise before the most rapid loss phase begins — which means clinicians who wait until postmenopause to screen for bone loss may already be behind.
The implication for women in perimenopause: bone health monitoring and preventive discussion should start during the transition, not after menopause is confirmed. First-line interventions remain weight-bearing exercise, adequate calcium and vitamin D intake, avoiding tobacco and excessive alcohol, and — for those who qualify — bisphosphonates or other antiresorptive agents for established bone loss or high fracture risk.
Peptide-based bone intervention (teriparatide, PTH 1-34; abaloparatide) is an option specifically for severe osteoporosis and high fracture risk, not preventive use in perimenopause. These are injectable prescription medications with strict indication criteria and a 2-year cumulative treatment limit. Their use in a perimenopausal context would be highly unusual and requires specialist involvement. See the full breakdown in our teriparatide guide.
Collagen Peptides: Where the Evidence Goes and Where It Stops
Collagen peptides occupy a different position from the injectable peptide categories above. They are oral supplements, not prescription drugs; they have a genuine RCT record; and they address outcomes — skin elasticity, dermal density, some bone marker data — that are relevant to perimenopausal women even if no trial has specifically enrolled a perimenopause-only cohort.
The König et al. RCT in Nutrients (PMID 29337906) enrolled 131 postmenopausal women with age-related bone density reduction and randomized them to 5 g daily of specific collagen peptides or placebo for 12 months. The collagen group showed statistically significant improvement in spine T-score (+0.1 vs. -0.03, p=0.030) and femoral neck T-score (+0.09 vs. -0.01, p=0.003). The bone formation marker P1NP rose significantly in the collagen group (p=0.007); CTX-1 (resorption marker) rose in controls. These are surrogate marker results, not fracture endpoint data — bisphosphonates and teriparatide have fracture data; collagen peptides do not.
The skin evidence is better-powered and more replicated. Multiple RCTs across different formulations, doses (2.5 g to 10 g/day), and follow-up durations (4 to 24 weeks) have found significant improvements in skin hydration, elasticity, and dermal density in women aged 35-65. The broader skin evidence is detailed in our peptides for women over 40 guide.
What collagen peptides do not do: they do not reduce hot flashes, improve vasomotor symptom frequency or severity, alter FSH or estradiol levels, or substitute for HRT in any mechanistically plausible way. A collagen peptide is a food-derived protein supplement that provides specific amino acid ratios; it is not an endocrine intervention.
HRT: The Standard of Care for Vasomotor Symptoms
Hormone therapy remains the most effective treatment for moderate to severe vasomotor symptoms (hot flashes, night sweats) in eligible perimenopausal and early postmenopausal women. The North American Menopause Society's position statement on hormone therapy — most recently substantially updated in 2022 — states that for women under 60 or within 10 years of menopause onset without contraindications, the benefits of hormone therapy outweigh the risks for treatment of vasomotor symptoms and prevention of bone loss.
This is not a marginal or contested finding: the evidence base for HRT and vasomotor symptom relief is substantially stronger than for any peptide category discussed in this article. No oral supplement — collagen or otherwise — has demonstrated clinically meaningful reduction in hot flash frequency or severity.
The 2022 NAMS position also distinguishes between combined estrogen-progestogen therapy (for women with an intact uterus) and estrogen-only therapy (for those post-hysterectomy), acknowledges individual risk assessment requirements (history of breast cancer, venous thromboembolism, cardiovascular disease each modify the risk-benefit calculation), and notes that the decision is individualized — not categorical.
One point requires explicit emphasis: compounded "bioidentical hormone" preparations sometimes marketed as "peptide therapy" are not equivalent to FDA-approved hormone therapy formulations. They have not undergone the same efficacy and safety testing, and actual hormone content can vary from the labeled dose. For women who cannot or choose not to use HRT, non-hormonal prescription options for vasomotor symptoms — including fezolinetant (approved in 2023) and certain antidepressants — exist and should be discussed with a physician.

Frequently Asked Questions
Can I take collagen peptides while on HRT?
Nothing in the published literature suggests a pharmacological interaction between oral hydrolyzed collagen and estrogen-progestogen therapy. Collagen is digested to amino acids before absorption. Whether combining the two provides additive bone or skin benefit has not been tested in a head-to-head trial.
Will a GLP-1 agonist also help my hot flashes?
Current evidence does not support a meaningful effect of GLP-1 receptor agonists on vasomotor symptom frequency or severity. Some women report subjective improvement in hot flash perception, which may relate to weight reduction (higher adiposity is associated with more severe vasomotor symptoms), but this is not an established or reliably reproducible effect. GLP-1s remain a weight and metabolic intervention, not a hormonal one.
Should I get a DEXA scan during perimenopause?
Screening recommendations vary by clinical guideline and individual risk. Given that the fastest bone loss clusters in the 3-year window around the final menstrual period, discussing timing of a baseline scan with a physician during the transition — rather than waiting until postmenopause is confirmed — is reasonable.
Are there peptides specifically approved for perimenopause?
No. Teriparatide is approved for osteoporosis in postmenopausal women with high fracture risk, not perimenopausal bone protection. GLP-1 agonists are approved for obesity and type 2 diabetes. Collagen peptides are dietary supplements with no approved therapeutic indication.
What about thyroid function during perimenopause?
The thyroid-perimenopause overlap is real: hypothyroid symptoms (fatigue, weight gain, mood changes, sleep disruption) overlap substantially with perimenopausal symptoms, and subclinical hypothyroidism becomes more common in midlife women. A thyroid panel is a reasonable part of the workup for women with these symptoms. See our peptides for thyroid conditions article for the evidence on peptide use in thyroid contexts, which remains very limited.
Conclusion: A Framework for Decision-Making
Perimenopause is a moving hormonal target spanning years, not months, and the evidence-based interventions map onto specific symptoms rather than the transition as a whole.
For vasomotor symptoms: hormone therapy is the standard of care for eligible women. No peptide or supplement has evidence comparable to HRT here.
For perimenopausal weight gain with central adiposity: lifestyle modification is the starting point. For women who qualify by standard criteria (BMI thresholds plus comorbidity), GLP-1 receptor agonists are the most effective pharmacologic option available — but they are prescription medications requiring clinical oversight, carry pregnancy considerations, and have no perimenopause-specific trial data.
For bone density: the window of fastest loss surrounds the final menstrual period. Baseline assessment, calcium, vitamin D, and weight-bearing exercise are appropriate for most women. Bisphosphonates or teriparatide for established osteoporosis or high fracture risk require specialist evaluation. Collagen peptides show modest bone marker benefit in postmenopausal women but have no fracture endpoint data and are not a substitute for antiresorptive therapy in high-risk individuals.
For skin and connective tissue: oral collagen peptides have the most accessible evidence and the most favorable risk profile in this category. Five grams per day of specific collagen peptides, taken consistently for at least 12 weeks, is a reasonable evidence-based choice as a complement to (not substitute for) medical management of menopausal symptoms.
The broader category of "peptides for perimenopause" in supplement marketing — peptide complexes, hormone-modulating peptides, bioidentical hormone peptide blends — has essentially no human trial data supporting its use in this life stage and should be viewed with significant skepticism.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
