If you're taking a prescription medication and wondering whether it's safe to add an adaptogen, the honest answer is: it depends on the specific drug class, the specific adaptogen, and whether your prescriber knows about it — and most do not, unless you tell them. This article organizes what the clinical literature and two leading authoritative databases actually show, by medication class rather than by herb. You will find which adaptogens create real pharmacokinetic or pharmacodynamic risks with each drug category, what the underlying mechanism is, and how serious the concern is. You will also get a cross-reference table at the end, a plain-language FAQ, and a direct instruction to bring your supplement list to every prescriber visit.
Summary: the quick answer on adaptogens and medication safety
Short answer: Several common adaptogens have documented interactions with prescription drugs — some serious enough to require prescriber sign-off before use, others requiring only monitoring. St. John's Wort represents the most dangerous single interaction in this category (serotonin syndrome with SSRIs), but ashwagandha, rhodiola, eleuthero, and schisandra each carry specific concerns that most supplement labels do not mention.
Best for (those who may use adaptogens with caution): Healthy adults on no prescription medications, who use standardized extracts from brands with third-party testing, for defined durations of 8–12 weeks.
Not ideal for:
- Anyone on warfarin, DOACs, or antiplatelet agents without prescriber review
- Anyone on levothyroxine, methimazole, or other thyroid medications
- Transplant patients on tacrolimus or cyclosporine
- Anyone taking an SSRI, SNRI, or MAOI antidepressant (especially with rhodiola or St. John's Wort)
- Anyone on benzodiazepines or barbiturates (especially with ashwagandha)
- Anyone on digoxin (especially with eleuthero)
- Immunosuppressed patients on biologics or calcineurin inhibitors
Decision shortcut: If you take any daily prescription medication, use the cross-reference table in this article and share the result with your pharmacist before starting any adaptogen.
What you'll find in this guide
- How adaptogens interfere with medications: the two main mechanisms
- Thyroid medications
- Antidepressants: SSRIs, SNRIs, and MAOIs
- Anticoagulants and antiplatelet agents
- Immunosuppressants
- Diabetes medications
- Sedatives and benzodiazepines
- CYP450 substrates: the metabolism wildcard
- Antihypertensives
- Stimulants
- Cardiac medications: the eleuthero-digoxin case
- Master cross-reference table
- Frequently asked questions
How adaptogens interfere with medications: the two main mechanisms {#two-mechanisms}
Before organizing interactions by drug class, it helps to understand the two ways an herb can interfere with a prescription drug.
Pharmacodynamic interactions happen when two substances act on the same physiological pathway. If ashwagandha promotes GABAergic sedation and you also take a benzodiazepine that amplifies GABA signaling, the combined effect is stronger than either alone — not because ashwagandha changes how the drug is metabolized, but because both are pushing the same lever. Additive sedation, additive blood pressure reduction, and additive blood-glucose lowering all fall into this category.
Pharmacokinetic interactions happen when one substance changes how the body handles another. Cytochrome P450 enzymes in the liver metabolize the majority of prescription drugs. An herb that inhibits a specific CYP enzyme causes the drug to accumulate to higher-than-intended levels. An herb that induces (speeds up) an enzyme causes the drug to clear faster, reducing its effectiveness. Rhodiola inhibits CYP2C9 in humans — a clinically relevant finding for warfarin and phenytoin. St. John's Wort powerfully induces CYP3A4, reducing blood levels of a long list of substrates.
Think of CYP enzymes like a toll road. Some herbs slow down the toll booths, causing drug traffic to pile up. Others open extra lanes, clearing the drug before it reaches its target. Either way, the intended dose no longer does what the prescriber calibrated it to do. Whether the mechanism is pharmacodynamic or pharmacokinetic, the practical result is the same: the medication either over-delivers or under-delivers, and the prescriber needs to know about the adaptogen to adjust accordingly.
Thyroid medications {#thyroid-medications}
Drugs in this class: Levothyroxine (Synthroid, Levoxyl), methimazole, propylthiouracil (PTU), liothyronine (T3).
Adaptogens of concern: Ashwagandha, holy basil (Ocimum sanctum), eleuthero.
Ashwagandha and thyroid hormones
Ashwagandha is the most extensively documented adaptogen for thyroid interaction. Multiple case reports in the clinical literature show a consistent pattern: patients develop elevated thyroid hormone levels after adding ashwagandha, with normalization after stopping.
A 2022 case report (PMC9035336) described a 73-year-old woman with known primary hypothyroidism who had self-discontinued levothyroxine and substituted ashwagandha root extract for two years. She presented with supraventricular tachycardia at 173 BPM, suppressed TSH below 0.01 mcIU/mL, and confirmed Hashimoto's thyroiditis on antibody testing. Symptoms and lab values resolved fully within two weeks of stopping the supplement. The authors proposed that ashwagandha may stimulate T4 synthesis and release at the glandular level, and additionally noted that some commercial ashwagandha products contain detectable amounts of T3 and T4 — levels that could exceed replacement doses.
Per Memorial Sloan Kettering's integrative herbs database, ashwagandha may increase thyroxine levels, which is a direct concern for anyone on levothyroxine or methimazole.
Holy basil and thyroid hormones
A 1998 comparative study (PMID 9721597) in male mice showed that holy basil leaf extract at 0.5 g/kg for 15 days significantly decreased serum T4 concentrations. T3 levels were not significantly affected. This antithyroidic finding places holy basil on the watch list for anyone managing hypothyroidism with levothyroxine, since a T4-lowering herb working against a T4-replacement medication creates an antagonistic interaction.
Eleuthero and thyroid function
The NCCIH ashwagandha fact sheet and related databases list thyroid hormone replacement therapies as a class of medications warranting caution with immune-modulating adaptogens generally. Eleuthero, which stimulates immune activity, also carries an unresolved question about thyroid interaction in susceptible populations.
Actionable takeaway: Anyone on levothyroxine, methimazole, or any thyroid drug should not add ashwagandha, holy basil, or eleuthero without informing their endocrinologist and arranging thyroid function monitoring.
Antidepressants: SSRIs, SNRIs, and MAOIs {#antidepressants}
Drugs in this class: Sertraline, fluoxetine, escitalopram, venlafaxine, duloxetine (SSRIs/SNRIs); phenelzine, tranylcypromine, selegiline (MAOIs).
Adaptogens of concern: St. John's Wort (severe — avoid), rhodiola (caution).
St. John's Wort: the most serious interaction in this category
St. John's Wort (Hypericum perforatum) is sometimes classified as an adaptogen in popular media, though its evidence base is primarily as a mild antidepressant. Regardless of classification, its interaction with serotonergic antidepressants is the most dangerous herb-drug interaction covered in this article.
The mechanism is dual. First, St. John's Wort inhibits reuptake of serotonin, dopamine, and norepinephrine — an action that overlaps directly with SSRIs and SNRIs. Second, it powerfully induces CYP3A4 and P-glycoprotein, which accelerates the clearance of many psychiatric medications. Per a 2023 clinical review (NBK557465), combining St. John's Wort with SSRIs creates a meaningful risk of serotonin syndrome — a potentially life-threatening condition characterized by tachycardia, elevated blood pressure, hyperthermia, clonus, and agitation. Initial symptoms include diaphoresis, tremor, and mydriasis, and the condition can progress to fever above 106°F and rhabdomyolysis.
The combination also risks reducing the efficacy of co-administered psychiatric medications through CYP3A4 induction, meaning an antidepressant may be less effective while the serotonin risk paradoxically increases from St. John's Wort's own serotonergic activity.
Clinical guidance is unambiguous: do not combine St. John's Wort with any SSRI, SNRI, or MAOI. A two-week washout period is recommended before restarting SSRI therapy after stopping St. John's Wort.
Rhodiola and antidepressants
Rhodiola demonstrates mild MAO inhibitory activity in preclinical studies. Per Memorial Sloan Kettering's herbs database, this activity "may increase serotonergic side effects" when rhodiola is combined with prescription antidepressants. A case report cited in the database documented tachyarrhythmia in a 26-year-old woman who combined rhodiola with her antidepressant for three days.
The interaction is not in the same severity category as St. John's Wort, but the signal is documented. MSK's guidance is explicit: "Patients taking prescription antidepressant medications should use rhodiola with caution."
Actionable takeaway: St. John's Wort with any SSRI, SNRI, or MAOI is a hard avoid, not a caution. Rhodiola with antidepressants warrants prescriber review before starting.
Anticoagulants and antiplatelet agents {#anticoagulants}
Drugs in this class: Warfarin (Coumadin), rivaroxaban (Xarelto), apixaban (Eliquis), dabigatran, aspirin (antiplatelet), clopidogrel.
Adaptogens of concern: American ginseng (documented INR reduction), reishi (case reports of elevated INR), rhodiola (CYP2C9 inhibition affecting warfarin metabolism), holy basil (antiplatelet activity), lion's mane (mild in vitro antiplatelet activity).
American ginseng and warfarin: a documented RCT
The strongest clinical evidence in this category involves American ginseng and warfarin. A 2004 randomized, double-blind, placebo-controlled trial (Yuan et al., PMID 15238367, n=20) found that two weeks of American ginseng administration significantly reduced warfarin's anticoagulant effect. Peak INR decreased by a mean difference of -0.19 (95% CI, -0.36 to -0.07; P=0.0012) compared to placebo. Warfarin peak plasma levels and area under the curve were also reduced. The authors concluded that physicians should ask patients about ginseng use when managing anticoagulation therapy.
This is a pharmacokinetic interaction, likely mediated through induction of CYP2C9, which metabolizes S-warfarin. The direction of the effect — warfarin becoming less effective — means the clinical risk is under-anticoagulation, with increased thromboembolism risk in patients who rely on warfarin for stroke or clot prevention.
Reishi and anticoagulants: case reports of elevated INR
Reishi (Ganoderma lucidum) presents the opposite pattern. Per Memorial Sloan Kettering's reishi database entry, reishi may prolong INR, PT, and APTT. A reported case involved a hemodialysis patient on warfarin therapy whose INR elevated to 6.92 and 8.22 after ingesting two 500 mg reishi tablets — a serious over-anticoagulation signal. Reishi demonstrates antiplatelet and anticoagulant activity in vitro, and MSK explicitly states that patients on blood thinners such as warfarin should consult their healthcare provider before using reishi.
Rhodiola and warfarin: CYP2C9 inhibition
A 2016 randomized crossover clinical study (Hellum et al., PMID 26613955, n=13) found that 14 days of rhodiola (Arctic Root) produced a statistically significant 21% decrease in CYP2C9 activity in healthy volunteers (p=0.023). The effect was most pronounced in extensive metabolizers of CYP2C9. The authors noted this "might be clinically relevant during treatment with CYP2C9 substrates with a narrow therapeutic index, such as phenytoin and warfarin." Because warfarin's S-enantiomer is a CYP2C9 substrate, rhodiola may cause warfarin to accumulate to higher levels — a bleeding-risk direction opposite to the ginseng interaction.
Holy basil and antiplatelet concerns
Holy basil may slow blood clotting through platelet-related mechanisms. Standard clinical references note that combining holy basil with anticoagulants or antiplatelets (aspirin, clopidogrel, heparin, warfarin) increases the risk of bruising and bleeding.
Lion's mane: mild in vitro signal, limited clinical relevance
A 2019 in vitro study (PMID 31842490) tested eight edible mushroom species for antiplatelet effects and found that lion's mane demonstrated modest inhibition of ADP-induced platelet aggregation. The same study found that "none of the mushroom extracts altered the monitored coagulation parameters (prothrombin time, prothrombin ratio, and INR)." Lion's mane produced weaker antiplatelet activity than the study's leading candidates. Clinical relevance is low, but patients on anticoagulants should disclose all mushroom supplement use to their prescriber.
Actionable takeaway: Anyone on warfarin, a DOAC, or an antiplatelet drug should not start or stop any adaptogen without informing their prescriber — the interaction direction differs by herb, and INR monitoring may need adjustment in either direction.
Immunosuppressants {#immunosuppressants}
Drugs in this class: Tacrolimus, cyclosporine, mycophenolate, azathioprine, biologics (adalimumab, infliximab, etanercept).
Adaptogens of concern: Ashwagandha, eleuthero, reishi, schisandra.
This is a high-stakes category. Immunosuppressants are prescribed because the immune system must be deliberately suppressed — for transplant rejection prevention, autoimmune disease, or management of biologics-dependent inflammatory conditions. Adaptogens that stimulate immune activity directly work against this goal.
Per Memorial Sloan Kettering's ashwagandha database entry, ashwagandha's withanolides can modulate immune function. For transplant patients or anyone on calcineurin inhibitors (tacrolimus, cyclosporine), this immune-stimulating activity is a contraindication, not merely a caution.
Schisandra presents an additional pharmacokinetic risk for tacrolimus. A pharmacokinetic modeling study (PMID 35562875) investigated schisandrol A and schisandrol B (lignans from Schisandra chinensis) and their effects on tacrolimus exposure mediated via CYP3A4/5 inhibition. Related research has found that schisandra extracts dramatically decreased in vivo metabolism of tacrolimus, with reported increases in tacrolimus AUC by 7–12 fold and Cmax by up to 10 fold. Tacrolimus has a narrow therapeutic index — small increases in exposure can cause nephrotoxicity and toxicity signals that are difficult to distinguish from rejection.
Reishi's immune-stimulating properties create a similar pharmacodynamic concern. MSK notes that individuals taking immunosuppressive medications should consult their provider before using reishi. For transplant patients and anyone on calcineurin inhibitors or biologics, immune-stimulating adaptogens are effectively contraindicated unless the transplant team or rheumatologist has explicitly reviewed and approved concurrent use.
Diabetes medications {#diabetes-medications}
Drugs in this class: Metformin, insulin, sulfonylureas (glipizide, glyburide), DPP-4 inhibitors (sitagliptin).
Adaptogens of concern: Ashwagandha, holy basil, lion's mane.
The concern is pharmacodynamic: additive blood-glucose lowering. The risk is higher with sulfonylureas and insulin than with metformin, because sulfonylureas and insulin can cause hypoglycemia where metformin typically does not.
Ashwagandha has demonstrated blood-glucose reduction in animal models and some human studies. Drug interaction databases list an additive hypoglycemia signal with metformin and insulin, though no published case reports of serious hypoglycemia from the combination exist in the current literature.
Holy basil showed antihyperglycemic effects in a 2008 clinical trial (Bhattacharyya et al., PMID 19253862). Lion's mane reduced serum glucose and raised serum insulin in a 28-day diabetic rat study (PMC3852124); human evidence is not established. Anyone on insulin or sulfonylureas should tell their prescriber which adaptogens they use and discuss whether more frequent glucose monitoring is warranted.
Sedatives and benzodiazepines {#sedatives}
Drugs in this class: Benzodiazepines (alprazolam, diazepam, lorazepam, clonazepam), barbiturates, non-benzodiazepine sleep aids (zolpidem, eszopiclone), anticonvulsants.
Adaptogens of concern: Ashwagandha.
Ashwagandha appears to have sedative and GABAergic properties — preclinical studies suggest it positively affects gene expression of the GABAA receptor subunit and may enhance GABA-mediated signaling. Per Memorial Sloan Kettering's database, patients who take benzodiazepines, anticonvulsants, or barbiturates should "likely avoid ashwagandha" because it may amplify CNS depression.
The interaction is pharmacodynamic — ashwagandha and the benzodiazepine are both increasing GABAergic inhibition, with potentially stronger combined sedation than either alone. Robust human trials on this combination have not been conducted, but the preclinical signal and the MSK guidance are sufficient to warrant prescriber disclosure, particularly for anyone who drives or operates machinery.
CYP450 substrates: the metabolism wildcard {#cyp450}
Relevant enzymes: CYP2C9, CYP3A4.
Adaptogens of concern: Rhodiola (CYP2C9 inhibitor — clinical evidence), schisandra (CYP3A4 inhibitor for tacrolimus, CYP3A4 inducer for warfarin), ashwagandha (modest CYP3A4 activity in vitro).
The cytochrome P450 system is how the liver metabolizes most prescription drugs. When an herb changes CYP enzyme activity, it can affect any drug on the same metabolic pathway.
Rhodiola and CYP2C9: The 2016 clinical crossover study (PMID 26613955) established that rhodiola produces a 21% reduction in CYP2C9 activity in humans. CYP2C9 substrates with narrow therapeutic indices include warfarin (S-enantiomer), phenytoin, and some NSAIDs. Inhibition means these drugs accumulate to higher blood levels. For warfarin, that means increased bleeding risk. For phenytoin, that means increased toxicity risk at unchanged doses.
Schisandra and CYP3A4: Schisandra presents a complex interaction profile. Research shows it inhibits CYP3A4-mediated metabolism of tacrolimus (potentially increasing tacrolimus levels 7–12 fold in animal models, with human modeling studies confirming the concern). Yet for warfarin, schisandra has been shown to act as a CYP3A4 inducer — potentially reducing warfarin's effectiveness and increasing clot risk. The same herb can increase some drug levels and decrease others depending on the specific metabolic pathway and drug involved.
Ashwagandha and CYP3A4: MSK notes that ashwagandha functions as a moderate CYP3A4 inducer in in vitro studies, which could theoretically reduce concentrations of drugs metabolized by this pathway. Human clinical significance has not been established, but the interaction is listed as a caution for drugs dependent on CYP3A4. CYP-mediated interactions are the most pharmacologically complex in this article: if you take any drug your pharmacist has described as having a "narrow therapeutic window," verify its CYP pathway before adding any adaptogen.
Antihypertensives {#antihypertensives}
Drugs in this class: ACE inhibitors, ARBs (losartan), calcium channel blockers, thiazide diuretics, beta-blockers.
Adaptogens of concern: Rhodiola, ashwagandha, holy basil.
The NCCIH lists antihypertensive medications among the drug classes warranting caution with ashwagandha. Rhodiola is specifically relevant to losartan: its CYP2C9 inhibition reduces losartan's conversion to its active metabolite EXP-3174, potentially weakening the antihypertensive effect. Per MSK, rhodiola's MAO inhibitory activity may also add to the hypotensive side effects of antihypertensive drugs. Home blood pressure monitoring during adaptogen use is reasonable for anyone in this drug class.
Stimulants {#stimulants}
Drugs in this class: Amphetamines (Adderall, lisdexamfetamine), methylphenidate (Ritalin, Concerta), modafinil.
Adaptogens of concern: Rhodiola, eleuthero.
Per MSK's herbs database, rhodiola's MAO inhibitory activity "may enhance the hypertensive effect" of CNS stimulants — a pharmacodynamic concern since both substances can raise blood pressure. Eleuthero's mild stimulating properties create a similar additive signal. People taking prescription stimulants for ADHD or narcolepsy should disclose adaptogen use to their prescriber and report new cardiovascular symptoms.
Cardiac medications: the eleuthero-digoxin case {#cardiac-medications}
Drug in question: Digoxin (Lanoxin).
Adaptogen involved: Eleuthero (Eleutherococcus senticosus, Siberian ginseng).
This interaction deserves its own section because its mechanism is uniquely confounding. A 1996 case report (PMID 8705908) described a 74-year-old man on digoxin whose serum digoxin levels elevated while taking Siberian ginseng, with levels normalizing after stopping and rising again when the herb was resumed. However, the study author explicitly stated that it was unclear whether the ginseng was converted to digoxin in vivo, interfered with digoxin elimination, or caused a false assay result.
Subsequent in vitro research on multiple ginseng preparations has confirmed that Siberian ginseng (eleuthero) interferes with several digoxin immunoassays, causing falsely elevated lab readings without necessarily changing actual digoxin pharmacology. A 2003 review (PMID 12580002) found that fluorescence polarization immunoassay (FPIA) — one of the most commonly used digoxin tests — is particularly susceptible to ginseng-related interference, while enzyme-linked chemiluminescent immunosorbent and turbidimetric assays are not.
The practical consequence: a patient taking eleuthero alongside digoxin may appear to have a dangerously elevated digoxin level — prompting dose reduction, hospitalization, or treatment changes — when their actual digoxin exposure is unchanged. This is an assay interference issue, but it carries identical clinical risk to a pharmacological interaction. Patients on digoxin should avoid eleuthero and all ginseng preparations, and must inform their cardiologist so the correct immunoassay method can be used for digoxin monitoring.
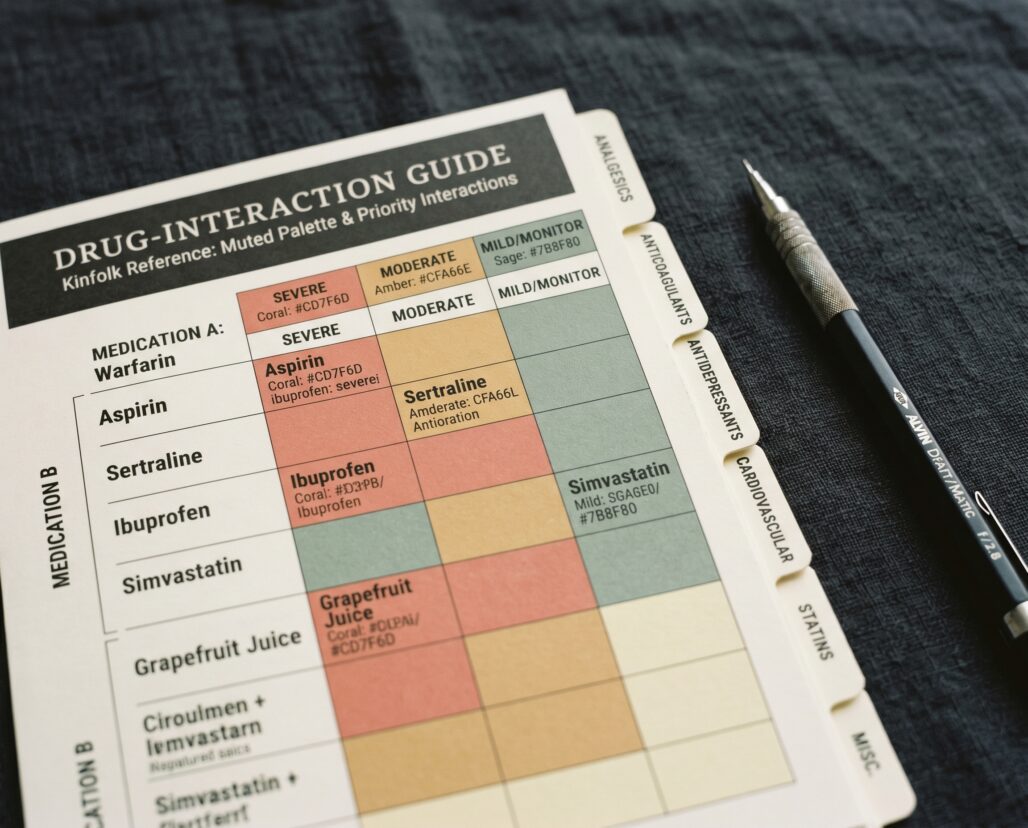
Master cross-reference table {#cross-reference-table}
Severity coding: AVOID = do not combine without specialist review; CAUTION = inform prescriber, monitor; MONITOR = low-level concern, disclose and observe; blank = no documented interaction or interaction too limited to classify.
| Adaptogen | Thyroid meds | Antidepressants (SSRI/SNRI/MAOI) | Anticoagulants | Immunosuppressants | Diabetes meds | Sedatives/Benzos | CYP450 substrates | Antihypertensives | Stimulants | Cardiac (digoxin) |
|---|---|---|---|---|---|---|---|---|---|---|
| Ashwagandha | AVOID | — | MONITOR | AVOID | CAUTION | AVOID | CAUTION | CAUTION | — | — |
| Rhodiola | — | CAUTION | CAUTION | — | — | — | CAUTION | CAUTION | CAUTION | — |
| St. John's Wort | — | AVOID | CAUTION | — | — | — | AVOID | — | — | — |
| Holy basil | CAUTION | — | CAUTION | — | CAUTION | — | — | CAUTION | — | — |
| Eleuthero | CAUTION | — | — | CAUTION | — | — | — | — | CAUTION | AVOID |
| Schisandra | — | — | CAUTION | AVOID | — | — | AVOID | — | — | — |
| Reishi | — | — | CAUTION | CAUTION | — | — | MONITOR | — | — | — |
| Lion's mane | — | — | MONITOR | — | MONITOR | — | — | — | — | — |
| Panax / American ginseng | — | — | CAUTION | — | MONITOR | — | CAUTION | — | — | — |
Table reflects documented interactions from NCCIH, MSK integrative herbs database, and primary clinical literature. Absence of a rating does not mean absence of interaction — it means insufficient published data as of 2026. The full interactions guide at usefulvitamins.com/complete-guide-to-adaptogens covers background safety profiles for each herb.
Frequently asked questions {#frequently-asked-questions}
Can I take adaptogens if I'm on blood pressure medication?
Possibly, but with prescriber awareness. Ashwagandha and holy basil may add blood-pressure-lowering effects. Rhodiola can reduce the efficacy of losartan through CYP2C9 inhibition. The NCCIH explicitly lists antihypertensive medications as a class of concern with ashwagandha. Disclose the specific adaptogen and your blood pressure drug class to your prescriber before starting.
Is it safe to combine ashwagandha and levothyroxine?
No — not without prescriber involvement and thyroid function monitoring. Multiple published case reports document thyrotoxicosis from ashwagandha in patients with thyroid conditions. The proposed mechanism involves both direct stimulation of thyroid hormone release and possible T3/T4 content in some commercial supplements. If you are on levothyroxine and want to trial ashwagandha, discuss with your prescribing physician and arrange TSH monitoring.
What is the most dangerous adaptogen-drug combination?
St. John's Wort with any SSRI or SNRI. The combination creates a meaningful risk of serotonin syndrome — a potentially life-threatening condition — through both pharmacodynamic overlap (both substances raise serotonin activity) and pharmacokinetic interaction (St. John's Wort CYP3A4 induction reduces SSRI levels while its own serotonergic activity continues). This combination is an avoid, not a monitor.
Should I stop my adaptogens before surgery?
Yes. The NCCIH notes ashwagandha should be avoided before surgery. Adaptogens with antiplatelet activity (reishi, holy basil, lion's mane) may prolong surgical bleeding. Standard guidance is to discontinue all supplements at least two weeks before a scheduled procedure.
Do all adaptogens interact with antidepressants?
No — but some do in clinically meaningful ways. Rhodiola's mild MAO inhibitory activity creates a caution with SSRIs and SNRIs. St. John's Wort's interaction is severe and well-documented. Most other adaptogens — ashwagandha, eleuthero, reishi, lion's mane — do not have documented interactions with antidepressants in the current literature, though absence of evidence is not evidence of absence.
Is there an adaptogen that is safe for everyone on medications?
No adaptogen has been formally studied across all medication combinations. Use the cross-reference table in this article as a starting point, then verify with your pharmacist or prescriber for your specific drug class.
Related reading
- For the full background on each adaptogen's evidence base and mechanism, see the Complete Guide to Adaptogens: What the Research Actually Shows in 2026
- For a full list of adverse effects beyond drug interactions, see Adaptogen Side Effects: The Master List for 2026
- For safety considerations specific to pregnancy, see Adaptogens During Pregnancy: What Is and Is Not Safe
Conclusion: the bottom line on adaptogens and medications
Adaptogens occupy a regulatory gray zone. They are sold over the counter, marketed as "natural," and rarely labeled with the drug interaction information that a clinical prescriber would need. That gap between supplement marketing and clinical reality is the problem this article addresses.
The interactions documented here are not theoretical. They include an RCT showing American ginseng reduces warfarin's effect, a 1996 case report of eleuthero producing falsely elevated digoxin levels, a 2022 case report of ashwagandha causing supraventricular tachycardia through apparent thyrotoxicosis, and a clinical crossover study showing rhodiola inhibits CYP2C9 at levels relevant to warfarin and phenytoin dosing. These are primary-source findings, not precautions invented by cautious label writers.
The single most important action you can take is to bring a written list of every supplement and adaptogen you use — brand name, dose, frequency — to every prescriber and pharmacist visit. That list does not need to be long. It needs to exist.
Next steps:
- Download or photograph the cross-reference table in this article before your next prescriber appointment
- If you take warfarin, digoxin, levothyroxine, an SSRI, or an immunosuppressant, use the table to identify your relevant row before starting any adaptogen
- Review the full safety profiles for any adaptogen you are considering in the Complete Guide to Adaptogens
This article is for informational purposes and not medical advice. Herbal adaptogens — even traditional ones — can interact with thyroid medication, antidepressants, anticoagulants, immunosuppressants, blood-pressure drugs, and more. Consult a licensed physician before starting any adaptogen, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
