Synthetic oxytocin is the same nine-amino-acid molecule whether it arrives in an IV bag hanging above a labor-and-delivery bed or in a small amber bottle mailed from a compounding pharmacy. The FDA-approved version, sold under the brand name Pitocin, has been used in hospital obstetric wards since the 1960s, backed by decades of clinical data on exactly one indication: stimulating uterine contractions under physician supervision. The intranasal formulation marketed to consumers for bonding, social anxiety, or autism support is a completely different regulatory story. It is compounded, meaning it left a pharmacy without any clinical trial package, and the human evidence behind its marketed uses is considerably thinner than the marketing suggests. The honest summary is not that oxytocin is a bad molecule. It is that the label on the bottle tells you very little about what the research actually found.
Summary / Quick Answer
Synthetic oxytocin has one FDA-approved indication: labor induction and uterine stimulation, administered intravenously in a hospital under physician supervision (Pitocin, NDA 018261). Intranasal oxytocin for bonding, autism, or social anxiety is compounded only and carries no FDA approval for any of those uses.
- What's approved: IV oxytocin (Pitocin) for labor induction, labor augmentation, and postpartum hemorrhage control, administered exclusively in a hospital setting.
- What's compounded: Intranasal oxytocin spray, produced by compounding pharmacies for off-label uses including social bonding, autism spectrum disorder, and social anxiety. Not FDA-approved for any of these indications.
- What the trials found: Large Phase 3 autism trials have largely failed to show benefit. Couples-bonding research consists primarily of small studies with significant replication problems and modest or inconsistent effect sizes.
- Decision shortcut: If someone is recommending intranasal oxytocin for a social or behavioral purpose, ask for the name of the randomized controlled trial with a sample size over 200 that showed benefit. You will usually get a reference to a small, unreplicated study.
Synthetic Oxytocin: The First Synthesized Peptide Hormone
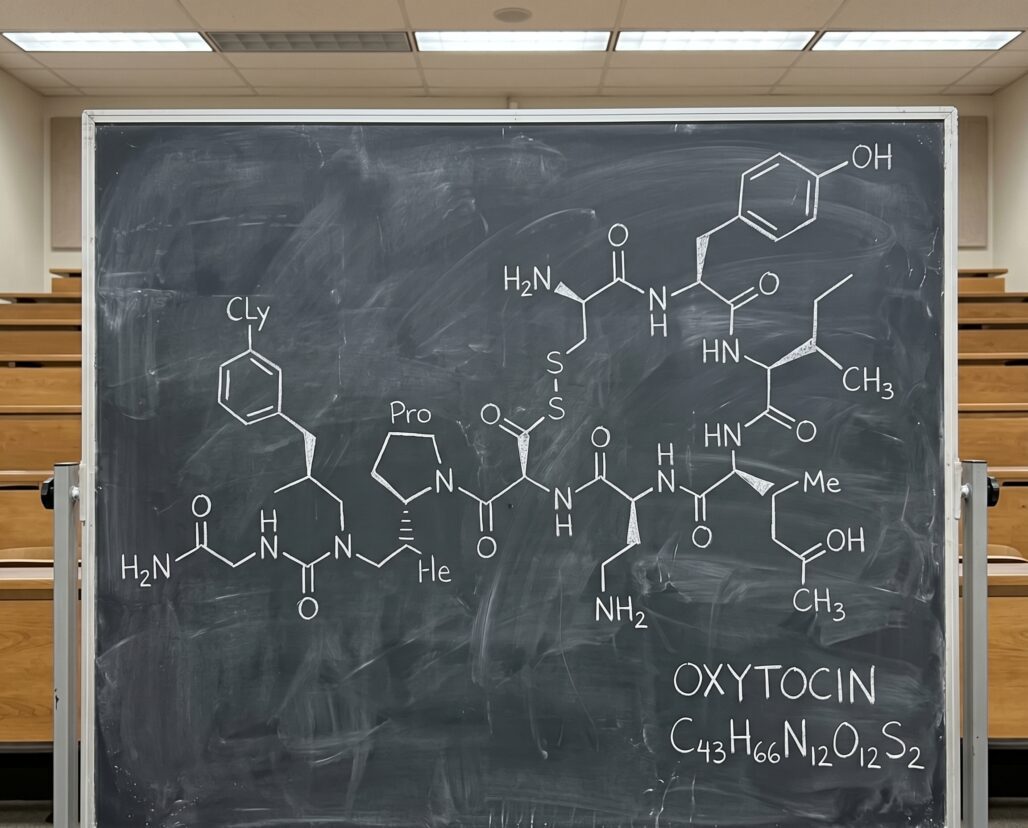
The history of synthetic oxytocin begins at Cornell University in 1953, when biochemist Vincent du Vigneaud and his team determined the complete amino acid sequence of oxytocin, a nine-amino-acid peptide produced by the posterior pituitary gland. Du Vigneaud's group identified the sequence and then achieved the first total chemical synthesis of any peptide hormone, a landmark that PMID 13129273 documents as the structure proposal for oxytocin with a proposal for its arrangement. The achievement was decisive enough that the Nobel Committee awarded du Vigneaud the 1955 Nobel Prize in Chemistry for his work on "biochemically important sulphur compounds, especially for the first synthesis of a polypeptide hormone," as the Nobel citation records it. Oxytocin was the first.
The molecule itself is compact by peptide standards: nine amino acids in a ring structure, with a disulfide bridge between cysteine residues at positions one and six. That ring structure distinguishes oxytocin from its close evolutionary cousin vasopressin, which differs by only two amino acids. The compact size made it the first feasible target for total synthesis with 1953-era chemistry.
The natural hormone is produced in the hypothalamus and released from the posterior pituitary in response to physiological stimuli including nipple stimulation during breastfeeding, cervical dilation during labor, and social touch. Its peripheral effects include uterine contraction and milk let-down. Its central effects, where the grey-market marketing enters, are more complicated and more contested. Understanding the what are peptides context matters here: being a naturally occurring peptide does not mean a synthetic dose produces the same effect, especially when the route of delivery changes.
Pitocin: What FDA Approval Actually Covers
The FDA-approved prescribing information for Pitocin (oxytocin injection, 10 units/mL, NDA 018261) lists the approved indications clearly. For antepartum use: the initiation or improvement of uterine contractions in patients with specific medical indications, including Rh problems, maternal diabetes, preeclampsia, and uterine inertia. As an adjunct for managing incomplete or inevitable abortion. For postpartum use: producing uterine contractions during the third stage of labor and controlling postpartum hemorrhage.
The label is equally explicit about what is not approved. Elective induction of labor, meaning induction without a recognized medical indication, is explicitly stated to lack adequate safety data and is not an approved use.
The route matters as much as the indication. Pitocin is for intravenous administration only in the context of labor induction. It is administered in a hospital, titrated carefully by clinical staff, and monitored continuously because the risk profile without that supervision is not theoretical. The label documents risks including uterine rupture, fetal distress, water intoxication from the antidiuretic effects of oxytocin at high doses, and maternal and fetal death. These are not the risks of a molecule that behaves gently. They are the risks of a potent uterotonic agent that has been well-characterized precisely because it has been studied at scale.
The mechanism is well understood: oxytocin binds to oxytocin receptors on uterine smooth muscle, increases intracellular calcium, and activates the contractile protein actomyosin. Receptor concentration in the uterus rises dramatically during late pregnancy, reaching its maximum near term, which is why the same dose produces far more powerful contractions at 40 weeks than at 20. This receptor-density sensitivity is one reason that clinical dosing protocols require careful titration starting from the lowest effective dose.
Takeaway: Pitocin is a legitimate, well-studied, and rigorously regulated obstetric drug. Its approval tells you nothing about intranasal oxytocin for social bonding, because those are different routes, different doses, different populations, and different proposed mechanisms in a different tissue. The molecule being the same does not make the evidence base the same.
Intranasal Oxytocin: Compounded, Off-Label, and Not FDA-Approved for Any Behavioral Indication
The idea that intranasal oxytocin could enhance social bonding, reduce anxiety, or improve autism symptoms grew from animal research showing that oxytocin signaling in the brain modulates social behavior in prairie voles and rodent models, and from initial small human studies in the early 2000s that suggested some effect on trust, eye contact, and social recognition. The concept was plausible, the early results were interesting, and the media coverage of "the love hormone" followed quickly.
Intranasal oxytocin is not FDA-approved for any indication in the United States. Products sold to consumers as oxytocin nasal sprays are compounded preparations, produced by a compounding pharmacy for an individual patient on the basis of a prescription, or sold through grey-market channels that lack even that minimal safeguard. The fda-approved-peptides article covers what compounding means in detail: compounded does not equal FDA-approved, does not equal quality-controlled in the way a branded drug is, and does not mean the dose on the label matches what is in the vial. The compounding pathway was not designed to create a consumer market for a behavioral supplement that never passed a Phase 3 trial.
Autism Trials: The Phase 3 Failure That Changed the Field
The clearest signal about where intranasal oxytocin stands in autism research comes from the largest trial ever conducted on the question. In 2021, Sikich and colleagues published results from a multicenter, randomized, double-blind, placebo-controlled trial of intranasal oxytocin in children and adolescents with autism spectrum disorder (PMID 34644471, N Engl J Med, 385:1462-1473). The study enrolled 290 participants aged 3 to 17 across institutions including Duke, Harvard, Columbia, and Mount Sinai. It was the definitive Phase 3 test of whether intranasal oxytocin could improve social function in pediatric ASD.
The trial failed to show a benefit on the primary outcome. Intranasal oxytocin did not outperform placebo on the Social Responsiveness Scale, the pre-specified primary endpoint. This was not a borderline result or a matter of statistical power. It was a well-powered, well-designed trial that produced a null finding.
The Sikich et al. result was not an isolated failure. Other trials in autism have shown similarly mixed or negative results. A 2020 randomized trial by Yamasue and colleagues (PMID 29955161) examining intranasal oxytocin in adults with high-functioning autism also did not find a significant difference in core social symptoms on the pre-specified primary measure. A 2023 randomized trial by Guastella and colleagues in young children with autism (PMID 36302965) concluded that its findings "suggest the need for further investigation" — careful language that communicates the absence of clear efficacy.
The pattern across these trials points to a consistent problem: the initial small studies that generated the hypothesis were almost certainly underpowered and subject to the same replication issues that afflicted social neuroscience broadly in the 2010s. Publication bias toward positive results created a literature that looked more supportive of intranasal oxytocin than it actually was.
The oxytocin system is genuinely relevant to social behavior, and this is not a reason to conclude the molecule plays no role in autism biology. But the hypothesis that exogenous intranasal oxytocin can correct that system meaningfully — at doses that traverse the nasal route — has not held up to rigorous testing.
Couples-Bonding Research: Small Studies and a Replication Crisis
The "bonding spray" marketing draws on a body of research involving intranasal oxytocin in healthy couples and individuals. The literature exists and is genuinely interesting. The conclusions vendors apply to it are considerably overstated.
A 2021 randomized crossover study (PMID 33601928) found that intranasal oxytocin may reduce jealousy-related responses in relationship scenarios; a 2019 study (PMID 30378456) found effects on social attention. These findings are real. What they are not is a demonstration that a compounded spray purchased online will produce meaningful relationship improvement. The studies are small, often using single doses in controlled lab conditions. Effect sizes are modest. Replication across independent laboratories has been inconsistent.
The deeper scientific problem is that intranasal delivery may not reliably increase oxytocin in the central nervous system. Oxytocin is a large, hydrophilic molecule that does not easily cross the blood-brain barrier. The nose-to-brain pathway some researchers propose — through olfactory and trigeminal nerves — has not been confirmed as the primary mechanism. Peripheral effects, placebo responses, and context effects are all plausible explanations for positive findings in small bonding studies, and larger pre-registered replications have often not reproduced early results cleanly.
Oxytocin is a fascinating molecule with a real role in mammalian social behavior, and the research is worth following. A compounded spray purchased for home use outside a research protocol is a speculative consumer product with an evidence base that has not held up to rigorous replication.
Takeaway: The interesting small studies are not the product you are buying. The product you are buying is a compounded preparation with no oversight and no replicated Phase 3 evidence behind the claims on the bottle.
Cost, Access, and Safety Profile
Compounded intranasal oxytocin is available through telehealth platforms and compounding pharmacies in the United States, typically requiring a prescription and generally priced between $50 and $150 per bottle. Some grey-market vendors sell it without a prescription at all.
The short-term safety profile in healthy adults at research doses (typically 18 to 40 IU intranasally) has not flagged serious adverse events in published trials. However, several caveats apply that the vendor's website will not mention.
Compounded preparations are not quality-controlled in the way FDA-approved drugs are. The actual oxytocin content, sterility, and preservative composition of any compounded product are not independently verified. "Compounded" can mean very different things depending on whether a pharmacy is an accredited 503A or 503B facility or a less-regulated operation.
Long-term safety data for chronic off-label intranasal use does not exist. The trials that established a short-term safety record used defined doses, durations, and active participant monitoring — conditions that home use without physician oversight does not replicate.
People with postpartum depression should not manage that condition with an unregulated spray; that is a serious clinical situation requiring an OB-GYN. The FDA has not issued a specific public warning about consumer intranasal oxytocin, but the absence of an approved product is itself the regulatory signal.

FAQ
Is Pitocin the same molecule as the oxytocin spray sold online? Yes, both are synthetic oxytocin — the identical nine-amino-acid peptide hormone. What differs radically is the formulation, the dose, the route of administration, the regulatory status, the quality controls, and the evidence base behind each product. Pitocin is an FDA-approved IV drug for obstetric use under physician supervision. Compounded intranasal oxytocin has no FDA approval for any indication.
Did intranasal oxytocin fail all autism trials? Not all trials showed zero effect, but the largest and most rigorous ones have not shown benefit on pre-specified primary outcomes. The Sikich et al. 2021 NEJM trial (PMID 34644471) is the most definitive study to date, and it was a null result. Smaller trials have produced mixed findings, which is the pattern you see when early positive results are generated by underpowered studies and later pre-registered replication attempts fail to confirm them.
Is it legal to buy intranasal oxytocin without a prescription? Purchasing compounded oxytocin without a prescription from a grey-market vendor is legally and medically problematic. Compounding is supposed to occur in response to a valid physician-patient relationship. Buying without a prescription bypasses that system entirely, leaving no way to verify what is in the product.
Can a doctor prescribe oxytocin off-label as a nasal spray? A physician can write a prescription for compounded intranasal oxytocin and a compounding pharmacy can prepare it. This is off-label use of a compounded preparation, not off-label prescribing of an FDA-approved drug — an important regulatory distinction. A physician who prescribes it responsibly should do so in a structured monitoring context.
What about oxytocin for postpartum depression? Postpartum depression is a serious clinical condition. Intranasal oxytocin has no established evidence base or FDA approval for it. Anyone experiencing postpartum depression should contact their OB-GYN or a mental health professional — not self-administer an unregulated spray.
If you are managing a protocol like this, StackMyMed (our companion app) keeps your doses, timing, and interaction checks in one place. It does not replace medical advice — bring the log to your clinician.
Conclusion: The Molecule Is Not the Product
Synthetic oxytocin has a legitimate and important role in obstetric medicine. The du Vigneaud synthesis in 1953 — the first total synthesis of any peptide hormone and the work that earned the 1955 Nobel Prize in Chemistry — made it possible to produce oxytocin at scale. That achievement gave medicine Pitocin, a drug that has saved maternal and neonatal lives in the context of carefully supervised labor management for decades.
The grey-market intranasal bonding spray sitting in the same molecular family as Pitocin is a different story. It carries the same molecule into a consumer market with none of the clinical evidence, quality controls, or physician supervision that makes the IV version a legitimate medical tool. The autism trials that were supposed to validate the spray's most compelling proposed use have largely failed to show benefit. The couples-bonding literature that generates the marketing copy consists of small, inconsistently replicated studies that have not scaled to clinical proof of concept.
This is not a call to dismiss oxytocin research entirely. The science of how this molecule modulates social behavior is genuinely interesting and still evolving. The call to dismiss is aimed at the gap between that ongoing science and the consumer product that vendors are already selling based on it.
If you are weighing a compounded oxytocin spray, the actionable question is this: which peer-reviewed trial with a sample size over 200 demonstrated the specific outcome you are hoping for, and what did the effect size actually mean in practical terms? Those questions, asked honestly, tend to reduce the appeal of the spray considerably — which is exactly the kind of accounting the label will never do on your behalf.
This article is for informational purposes only and does not constitute medical advice. Synthetic oxytocin (Pitocin) is an FDA-approved prescription drug for obstetric indications only, to be administered by healthcare professionals in a hospital setting. Compounded intranasal oxytocin is not FDA-approved for any indication. Nothing in this article should be interpreted as a recommendation to use, purchase, or discontinue any medication or compounded preparation. Always consult a qualified healthcare provider before making decisions about any treatment.
