If you or someone you care for has been prescribed Lupron — or if you have seen leuprolide mentioned in the context of prostate cancer, endometriosis, or early puberty in a child — you have probably wondered how a single drug ends up treating three conditions that appear to have nothing in common. The honest answer is that they share a common hormonal pathway, and leuprolide exploits that pathway with precision. The more complicated answer involves a counterintuitive mechanism: a drug that mimics a hormone so aggressively that it eventually shuts off the body's production of that hormone entirely. That is not a side effect. It is the therapeutic goal.
Leuprolide (brand names: Lupron Depot, Eligard, and generics) is an FDA-approved synthetic peptide that reliably suppresses sex hormone production and has been used clinically since 1985 — making it one of the longest-standing peptide therapies in oncology and gynecology.
Summary
- Leuprolide is a synthetic analog of gonadotropin-releasing hormone (GnRH), a naturally occurring 10-amino-acid peptide; leuprolide has 9 amino acids and carries a modification that makes it far more potent than the native hormone.
- It works by initially triggering a surge in sex hormones, then desensitizing the pituitary so profoundly that hormone production collapses — a process called downregulation.
- The FDA has approved leuprolide for four distinct indications: advanced prostate cancer, endometriosis, uterine fibroids (pre-surgery), and central precocious puberty (CPP) in pediatric patients.
- Depot formulations allow dosing every 1, 3, 4, or 6 months depending on indication and formulation.
- The safety profile includes bone density loss with long-term use, a mandatory cardiovascular risk warning in men on androgen deprivation therapy, and an absolute contraindication in pregnancy.
- All three patient populations — men with prostate cancer, women with endometriosis, and children with CPP — require separate clinical considerations. They should not be conflated.
What Leuprolide Is: A Synthetic GnRH Analog
Peptides as a drug class span everything from insulin to GLP-1 receptor agonists. Leuprolide belongs to a smaller subcategory: synthetic analogs of endogenous hormones that regulate the reproductive axis.
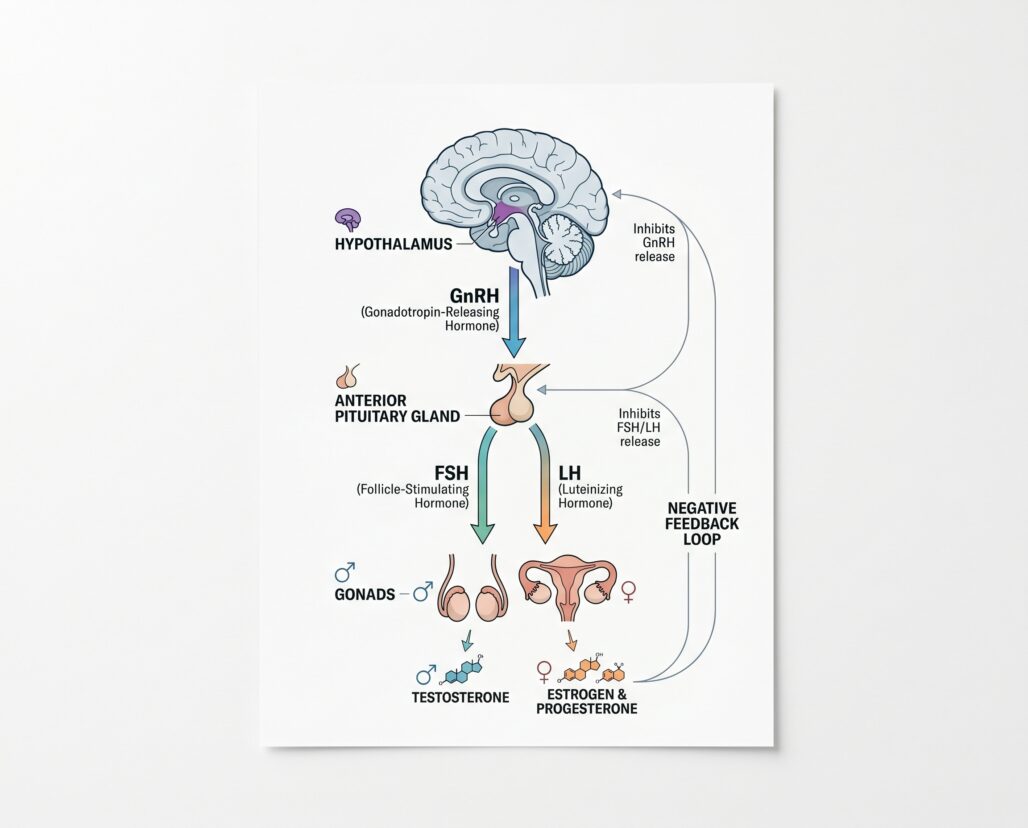
GnRH (gonadotropin-releasing hormone) is produced in the hypothalamus, a small region at the base of the brain. It travels a short distance to the pituitary gland, where it binds to GnRH receptors and triggers the release of two other hormones: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Those two hormones then travel through the bloodstream to the gonads — the testes in men, the ovaries in women — where they stimulate the production of testosterone and estrogen, respectively.
Leuprolide is a 9-amino-acid synthetic peptide with structural modifications at positions 6 and 10 relative to the native 10-residue GnRH sequence. The substitution at position 6 replaces L-glycine with a D-amino acid, which resists enzymatic breakdown and dramatically extends the molecule's half-life. The result is a compound that binds GnRH receptors with higher affinity than the natural hormone and persists far longer in tissue.
The FDA first approved leuprolide for advanced prostate cancer in 1985 under NDA 019943 and NDA 020011, originally by TAP Pharmaceuticals, which later became AbbVie. Subsequent approvals expanded the label to endometriosis, uterine fibroids, and CPP.
How It Works: The Flare-Then-Suppression Mechanism
This is the part that surprises most patients. A drug used to suppress sex hormones begins by causing a sharp, temporary spike in those very hormones. Understanding why requires understanding how GnRH normally works.
Under normal physiology, the hypothalamus releases GnRH in short, rhythmic pulses — roughly every 60 to 120 minutes. That pulsatile signal is what the pituitary is designed to detect and respond to. When GnRH arrives in a pulse, the pituitary releases LH and FSH. When the pulse subsides, the pituitary resets.
Leuprolide depot does the opposite of pulsatile. It delivers a prolonged, continuous signal to the pituitary's GnRH receptors. The pituitary initially interprets this as a very strong pulse and responds with a large release of LH and FSH — which then drives the gonads to produce sex hormones. This is the "flare" phase.
For men being treated for prostate cancer, the Lupron Depot prescribing information states this plainly: leuprolide causes "increases in serum levels of testosterone to approximately 50% above baseline during the first weeks of treatment." That initial testosterone surge can cause transient worsening of prostate cancer symptoms — bone pain, increased urinary obstruction, and, in patients with spinal metastases, a risk of spinal cord compression. This is not a minor footnote. Patients with vertebral metastases or significant urinary obstruction require especially careful monitoring during the first one to two weeks of treatment, and co-administration of an antiandrogen drug at initiation is standard clinical practice to blunt the flare.
After approximately one to two weeks of continuous GnRH receptor stimulation, the pituitary receptors become desensitized. They are still occupied, but they stop responding. The pituitary reduces its output of LH and FSH. The gonads receive no signal to produce testosterone or estrogen. Within two to four weeks of initiation — and reliably by the end of the first month — serum testosterone in men falls to castrate levels (generally below 50 ng/dL), and estrogen in women falls to post-menopausal levels. The drug has achieved, through receptor saturation and downregulation, the functional equivalent of surgical removal of the gonads — without surgery.
This suppression is reversible. When leuprolide is discontinued, GnRH receptors recover their sensitivity over months, and hormone levels typically return toward baseline. This reversibility is clinically significant, particularly for women with endometriosis who may wish to preserve fertility and for children with CPP where treatment ends at the appropriate developmental age.
Major Indications: Three Patient Populations, Three Separate Conversations
Leuprolide treats three very different patient groups. Conflating their experiences or risk profiles is a significant clinical error.
Advanced Prostate Cancer (Men, Typically 60+)
The most established use. Prostate cancer cells are testosterone-dependent; reducing testosterone to castrate levels slows tumor growth and can reduce PSA, shrink tumor bulk, and relieve symptoms in metastatic disease. Leuprolide does not cure prostate cancer. It suppresses hormone production to deprive the tumor of its growth signal, a strategy called androgen deprivation therapy (ADT).
Depot formulations approved for this indication include the 7.5 mg monthly, 22.5 mg every 3 months, 30 mg every 4 months, and 45 mg every 6 months formulations of Lupron Depot, as well as Eligard (leuprolide acetate for injectable suspension), which uses a different polymer delivery system but the same active molecule.
Men on ADT with leuprolide face specific long-term safety concerns that deserve direct acknowledgment. The prescribing information carries an explicit warning: "Increased risk of developing myocardial infarction, sudden cardiac death and stroke has been reported in association with use of GnRH agonists in men." This cardiovascular risk is not a theoretical signal — it reflects observations from large clinical datasets and has been incorporated into the FDA labeling for all GnRH agonists. Men with pre-existing cardiovascular disease or risk factors warrant careful monitoring and shared decision-making with their oncologist before initiating therapy.
Endometriosis (Women)
Leuprolide is approved for the management of endometriosis, including pain relief and reduction of endometriotic lesions. By suppressing estrogen to post-menopausal levels, it creates a hormonal environment that causes estrogen-dependent endometrial tissue outside the uterus to regress.
The 3-month Lupron Depot 11.25 mg formulation and the monthly 3.75 mg formulation are both indicated for this use. Treatment duration is limited — the prescribing information specifies a maximum of 12 months total due to bone mineral density concerns. For retreatment or extended use, "add-back therapy" with norethindrone acetate is co-prescribed to partially offset bone loss while maintaining enough estrogen suppression to control symptoms.
Two hard facts for women considering this therapy: first, pregnancy is absolutely contraindicated during treatment. Leuprolide may cause fetal harm based on animal studies and its mechanism of action; non-hormonal contraception is required during therapy. Second, the hot flashes, night sweats, mood changes, and other symptoms of estrogen suppression that occur during treatment are essentially medically induced menopause. They are expected, they are temporary, and they typically resolve after stopping the drug — but they can be significant during treatment.
The drug is also approved for preoperative improvement of anemia caused by uterine fibroids, in a short course alongside iron therapy, to shrink fibroid mass before surgery.
Central Precocious Puberty in Pediatric Patients
This is the indication that requires the most careful framing. Central precocious puberty (CPP) is defined as the onset of puberty — breast development, testicular growth, pubic hair, and the hormonal cascade that precedes growth plate fusion — before age 8 in girls and before age 9 in boys. When puberty begins this early, the growth plates in long bones accelerate their closure. A child who appears tall initially may end up shorter as an adult than their genetic potential would suggest, because their bones fused before they had time to grow further. CPP also carries psychological and social consequences for young children suddenly experiencing pubertal changes years before their peers.
Lupron Depot-PED is approved for CPP in patients as young as 1 year of age. Dosing is weight-based for the monthly formulation (7.5 mg for children weighing 25 kg or less, 11.25 mg for 25-37.5 kg, and 15 mg for over 37.5 kg), with additional 3-month (11.25 mg or 30 mg) and 6-month (45 mg) depot formulations available.
The mechanism in CPP is the same as in adults: continuous GnRH receptor stimulation causes pituitary downregulation, suppressing LH, FSH, and ultimately the gonadal sex steroids that are driving premature pubertal development. Clinical studies show that 96% of patients achieve LH suppression below 1.75 mIU/mL within the first month of therapy with the monthly formulation — a high rate of biochemical success.
A common and legitimate parental concern is: what does suppressing these hormones do to a developing child's bones? The prescribing information addresses this directly, citing published literature: bone mineral density may decrease during GnRH therapy in pediatric CPP patients. However, the data also show that "after discontinuation of therapy, subsequent bone mass accrual is preserved and peak bone mass in late adolescence does not seem to be affected." This is meaningfully different from the long-term bone loss seen with indefinite ADT in adult men. Monitoring with height measurements and bone age assessments every 6 to 12 months is standard.
The consistent position in the literature and from pediatric endocrinology societies is that CPP treatment with GnRH agonists is supported by evidence and considered standard of care — but it requires specialist supervision. A pediatric endocrinologist diagnoses CPP (which requires confirmation by hormonal testing and bone age X-ray), initiates treatment, and monitors response. This is not a condition that should be managed without that level of specialist involvement. For a broader look at why pediatric peptide use requires specialist oversight, that article covers the subject in detail.
Treatment ends at the clinically appropriate age — when it is determined that the child has reached an age where natural puberty is developmentally appropriate to proceed. Mean treatment duration in clinical studies was approximately four years.
Side Effects, Bone Density, and Cardiovascular Risk
The side effects of leuprolide are largely the predictable consequences of sex hormone deprivation. They differ by population.
In men on ADT for prostate cancer, the most consistent adverse effects include: hot flashes (reported in the majority of patients), decreased libido, erectile dysfunction, fatigue, muscle loss, weight gain (particularly visceral fat), and mood changes including depression. Bone mineral density loss begins within months of starting therapy and accumulates with continued treatment. Guidelines for men on long-term ADT recommend baseline DEXA scanning before or shortly after initiation, periodic repeat scans, calcium and vitamin D supplementation, and assessment for pharmacologic bone-protective therapy (bisphosphonates or denosumab) in patients at high fracture risk.
The cardiovascular risk mentioned in the prescribing information — myocardial infarction, sudden cardiac death, stroke — reflects a body of observational literature showing that men on GnRH agonists have higher rates of cardiovascular events than men with prostate cancer who are not on ADT. The mechanism is likely multi-factorial: metabolic effects of testosterone deprivation (increased adiposity, dyslipidemia, insulin resistance) combined with an older patient population that already carries significant cardiovascular burden. This does not mean that ADT is categorically contraindicated in men with cardiovascular disease — in many patients, the cancer risk clearly outweighs the cardiovascular risk — but it means the conversation must happen explicitly.
In women on leuprolide for endometriosis, the induced hypoestrogenic state produces hot flashes, vaginal dryness, headache, and mood changes alongside the bone density concern that limits treatment duration. The 12-month maximum is not arbitrary; it reflects the clinical judgment that beyond that duration, cumulative BMD loss reaches a threshold where the risk-benefit calculation shifts. Add-back norethindrone therapy significantly reduces this bone loss without substantially compromising endometriosis control.
In children with CPP, the most common adverse effects include injection site reactions, headache, emotional lability, and mood changes. The initial flare effect produces transient vaginal spotting or bleeding in approximately 19% of female patients in the first four weeks — which can be alarming for parents who were not warned to expect it. Postmarketing reports include psychiatric events and, rarely, convulsions and severe cutaneous adverse reactions.
Across all populations, anaphylaxis and serious hypersensitivity reactions have been reported post-marketing, as have rare cases of Stevens-Johnson syndrome. These are not common, but they underscore why leuprolide administration occurs in clinical settings or with appropriate patient education about warning signs.
The Pediatric CPP Nuance: What Parents Ask Most
Parents whose child has been diagnosed with CPP often arrive at the treatment conversation with understandable anxiety. Several points tend to clarify the picture.
First, the diagnosis of CPP itself is the result of a clinical evaluation — it is not a close call made casually. A child must meet published age thresholds, demonstrate hormone levels consistent with central (pituitary-driven) puberty rather than peripheral (gonadal) puberty, and typically show advanced bone age on wrist X-ray. GnRH stimulation testing may be performed to confirm the central origin. The diagnosis drives the treatment decision; the treatment does not happen before the diagnosis is established.
Second, the goal of treatment is not to prevent puberty. It is to pause it until an age-appropriate time. When treatment stops, puberty resumes. The vast majority of children who complete a course of GnRH agonist therapy for CPP go on to experience normal pubertal development, normal adult height, and normal fertility. The evidence base here extends to decades of follow-up data in treated cohorts.
Third — and this bears emphasis — no one should be administering leuprolide or any GnRH agonist to a child outside of a formalized relationship with a pediatric endocrinologist. This is not a drug available from grey-market sources for non-medical purposes. The off-label use of hormone-suppressing agents in children outside of a diagnosed medical condition is not supported by evidence and carries risks that are not acceptable. Any suggestion to the contrary should be met with immediate skepticism and referral to a qualified specialist.
Frequently Asked Questions
How is leuprolide different from other GnRH agonists like histrelin or triptorelin? They share the same mechanism — continuous GnRH receptor stimulation leading to pituitary downregulation — and produce similar clinical outcomes. The practical differences are in formulation, delivery system, approved indications, and duration between doses. Leuprolide has the broadest FDA approval record among GnRH agonists in the United States, partly because it has been on the market since 1985.
Does leuprolide cure prostate cancer? No. It is a hormone-suppressive therapy that slows the growth of testosterone-dependent prostate cancer. It is most effective in hormone-sensitive (also called castration-sensitive) prostate cancer. Once a tumor evolves to become castration-resistant — meaning it grows despite low testosterone — leuprolide alone is no longer the main treatment strategy and second-generation androgen receptor inhibitors or other agents take priority.
Can leuprolide be used off-label for gender-affirming hormone therapy? Leuprolide and other GnRH agonists are prescribed off-label as puberty blockers in the context of gender-affirming care for adolescents. This is a separate clinical and policy conversation from the FDA-approved CPP indication. The mechanism is the same — pituitary downregulation — but the patient population, clinical context, monitoring protocols, and current regulatory environment differ significantly. This article does not address or recommend any off-label use.
What monitoring is required during treatment? For prostate cancer: PSA and serum testosterone levels, bone density (DEXA) at baseline and periodically, cardiovascular risk assessment. For endometriosis: symptom assessment, bone density if treatment extends toward the 12-month limit or if retreatment is considered. For CPP: GnRH stimulation testing or basal LH levels at 1-2 months after initiation and with dose changes; height and bone age every 6-12 months; regular clinical assessment of pubertal status.
Is the cancer-risk concern from the peptides-and-cancer-risk article relevant here? The concern in that article focuses on unregulated peptides that may stimulate growth factor pathways indiscriminately. Leuprolide works in the opposite direction for its primary cancer indication — it suppresses, rather than stimulates, a hormonal growth signal. The risk profiles are categorically different.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Practical Takeaways
- If you are a man with prostate cancer starting leuprolide, ask your oncologist explicitly about the testosterone flare in the first one to two weeks and whether antiandrogen co-treatment is appropriate for your situation.
- If you are a woman on leuprolide for endometriosis, confirm your treatment duration with your gynecologist, ask about add-back therapy if you are experiencing significant side effects, and ensure you are using non-hormonal contraception throughout treatment.
- If your child has been diagnosed with CPP and leuprolide is being recommended, verify that the diagnosis was confirmed by a pediatric endocrinologist with appropriate hormonal testing and bone age assessment, and establish the monitoring plan before starting treatment.
- Across all three indications, bone density deserves attention. Do not wait until the end of treatment to have the conversation about DEXA monitoring and calcium/vitamin D intake with your prescribing physician.
Conclusion
Leuprolide has earned its place as one of the most versatile peptide drugs in clinical medicine — not through novelty but through decades of evidence across genuinely distinct medical conditions. Its mechanism is counterintuitive but well-established: by flooding the pituitary with a relentless hormonal signal, it paradoxically shuts down the very hormonal axis it mimics. The result is a reliable, reversible suppression of sex hormone production that is clinically useful in advanced prostate cancer, estrogen-driven endometriosis, and hormone-driven early puberty. The tradeoffs — bone density loss, cardiovascular risk in older men, the transient initial flare — are real and require active management, not dismissal. For the three populations it is designed to serve, leuprolide is among the most evidence-supported peptide therapies in the FDA's approval history. For anyone outside those populations, there is no evidence base and no legitimate clinical argument for its use.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
