You may have come across octreotide in a bodybuilding forum or a wellness thread with the vague framing that it "blocks GH" or helps with "spot reduction." That framing is worth pausing on, because octreotide is a serious prescription drug with a specific set of FDA-approved indications, a well-documented side-effect profile, and zero clinical evidence backing cosmetic body-composition use. Before deciding whether it belongs anywhere near your health decisions, it helps to understand what it actually does, in whom it was tested, and why the gap between the clinical reality and the internet mythology is wider than most people realize.
Octreotide is an FDA-approved, synthetic somatostatin analog used to treat acromegaly, carcinoid syndrome, and VIP-secreting tumors; it is not a body-composition drug, and no controlled clinical trial supports its use for fat loss or physique improvement.
Summary
- Octreotide (brand names Sandostatin and Sandostatin LAR) is a synthetic 8-amino-acid peptide that mimics the natural hormone somatostatin, suppressing growth hormone, glucagon, insulin, and several GI hormones.
- The FDA first approved octreotide in 1988 for acromegaly, carcinoid syndrome, and VIPoma. An oral capsule formulation (Mycapssa) received approval in 2020 for acromegaly maintenance.
- Gallstone formation occurs in up to 52% of patients on long-term therapy; this requires active monitoring, not passive acceptance.
- Glucose metabolism is altered in both directions: hypoglycemia and hyperglycemia are both documented adverse effects.
- No clinical evidence supports octreotide for cosmetic fat reduction or body recomposition. Off-label use for these purposes is without supporting trials.
What Octreotide Is: A Synthetic Somatostatin Analog
Natural somatostatin is a 14-amino-acid cyclic peptide produced primarily in the hypothalamus and pancreatic delta cells. Its job, broadly speaking, is to act as a brake on secretion: it slows the release of growth hormone from the pituitary, restrains insulin and glucagon from the pancreas, and damps down a long list of gastrointestinal hormones including gastrin, secretin, motilin, and VIP. Think of it as the body's internal volume-control knob for hormonal output, capable of dialing down multiple systems at once.
The problem with natural somatostatin as a drug is its half-life in the bloodstream: roughly 1 to 3 minutes. That makes it essentially useless for therapeutic purposes, since you would need a continuous infusion just to maintain any effect.
Octreotide was engineered to solve that problem. Developed in the early 1980s and first approved by the FDA in 1988 (NDA 019667), it compresses somatostatin's key functional sequence into an 8-amino-acid synthetic ring structure. Two amino acids were substituted to resist enzymatic breakdown, extending the half-life to approximately 100 minutes for subcutaneous injection. That is about 40 times longer than natural somatostatin, long enough to produce sustained clinical effects. The longer-acting depot formulation, Sandostatin LAR, takes that further by encapsulating the drug in biodegradable microspheres that release octreotide slowly over a four-week period, converting a multiple-daily-injection regimen into a single monthly intramuscular shot.
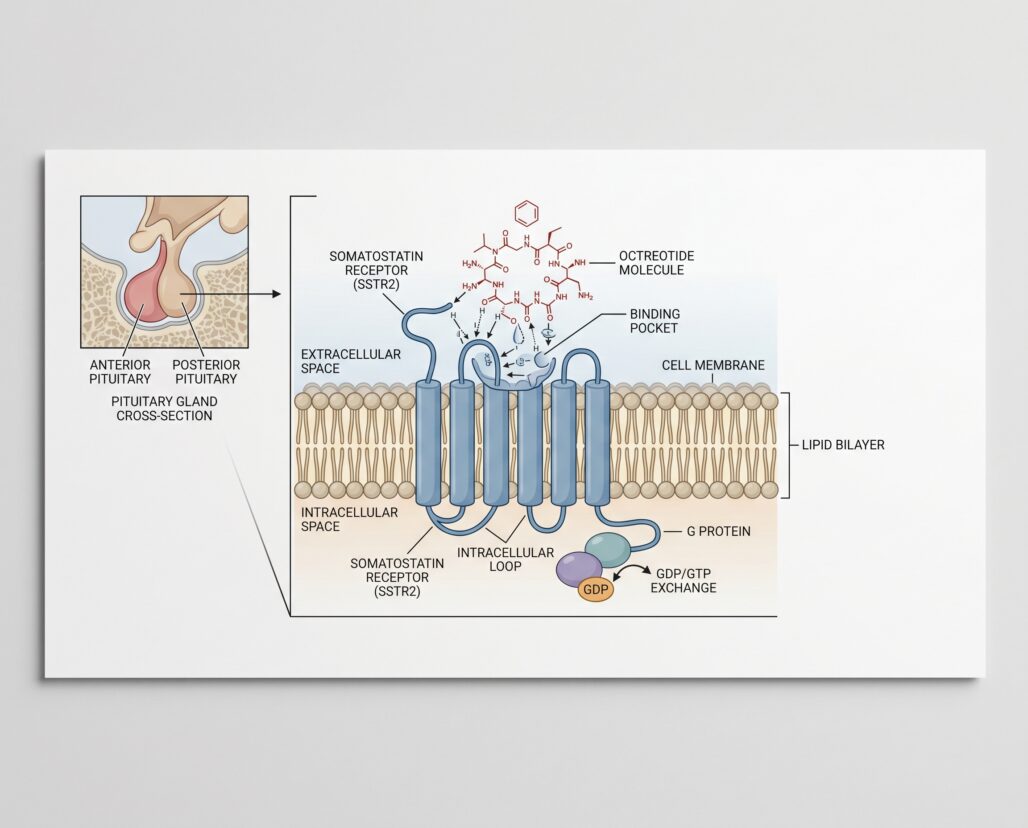
Octreotide's structural changes did more than extend its life: they also shifted its receptor selectivity. Natural somatostatin binds all five somatostatin receptor subtypes (SSTR1-5) roughly equally. Octreotide preferentially binds SSTR2 and SSTR5, the receptor subtypes most responsible for growth hormone suppression and GI hormone inhibition. That selective binding is why it works so well for its approved indications, and also why it does not reproduce every effect of natural somatostatin. It is a targeted tool, not a full somatostatin replacement.
FDA-Approved Indications
Octreotide carries three primary FDA-approved indications. This section covers each one with the clinical context that makes the approval understandable.
Acromegaly. Acromegaly is a condition caused by sustained excess growth hormone secretion, most often from a benign GH-secreting pituitary tumor (somatotroph adenoma). The results of untreated or undertreated acromegaly are serious: progressive enlargement of the hands, feet, and facial features, cardiovascular complications, joint damage, and a significantly elevated mortality risk compared to the general population. Surgery to remove the pituitary tumor is the primary treatment, but it does not achieve biochemical control in all patients. For those with persistent disease or incomplete surgical response, somatostatin receptor ligands like octreotide are the principal medical therapy. First-generation agents including octreotide LAR and lanreotide autogel achieve biochemical normalization of IGF-1 levels in approximately 40% of patients and produce tumor shrinkage in over 60% (PMID 34618894). Octreotide is not a cure. It is a management tool used when surgery is incomplete, when patients decline surgery, or while awaiting the effects of radiation therapy.
Carcinoid syndrome. Carcinoid tumors are neuroendocrine tumors that, when metastatic to the liver, secrete serotonin and vasoactive substances directly into systemic circulation, causing episodic flushing, profuse diarrhea, bronchospasm, and in advanced cases, carcinoid heart disease (PMID 28846309). Octreotide blunts this hormonal excess, providing meaningful symptom control. The FDA approval covers suppression of severe diarrhea and flushing; it does not imply a curative or tumor-shrinking effect.
VIPomas. VIP-secreting pancreatic neuroendocrine tumors (VIPomas) cause Verner-Morrison syndrome: profuse watery diarrhea, hypokalemia, and achlorhydria. Fluid losses can reach several liters daily, creating life-threatening electrolyte disturbances. Octreotide suppresses VIP secretion and reduces diarrheal volume, stabilizing patients for further treatment.
One additional clinical use worth noting: octreotide is widely deployed in acute variceal hemorrhage, bleeding from esophageal varices caused by portal hypertension in cirrhosis. IV octreotide reduces splanchnic blood flow and portal pressure alongside endoscopic intervention. A 2021 meta-analysis of 21 randomized controlled trials found octreotide and somatostatin comparable to terlipressin and vasopressin for bleeding control, with a better tolerability profile (PMID 33723542).
Mechanism: Multi-Receptor Somatostatin Agonism
Understanding octreotide's mechanism explains both its clinical utility and its side-effect profile. By preferentially activating SSTR2 receptors on somatotroph cells in the pituitary, octreotide suppresses GH synthesis and release, which in turn reduces liver production of IGF-1, the downstream mediator responsible for most of acromegaly's tissue effects.
Simultaneously, SSTR2 and SSTR5 activation in the pancreas restrains both glucagon and insulin release. This dual suppression of counterregulatory hormones creates the drug's glucose metabolism effects, discussed in more detail in the side-effects section below. In the GI tract, the same receptors slow gut motility, reduce intestinal fluid secretion, and cut the output of multiple regulatory peptides. This is why octreotide is so effective for secretory diarrheas driven by carcinoid syndrome or VIPoma, but it is also why GI side effects are the most common complaint in patients receiving the drug.
Forms and Dosing
Octreotide is available in three distinct formulations, each with a different clinical role.
Subcutaneous injection (Sandostatin, immediate-release). This is the original formulation used to initiate therapy. Acromegaly dosing starts at 50 micrograms three times daily, titrated to a maintenance range of 100 to 500 micrograms three times daily based on GH and IGF-1 response. Carcinoid syndrome starts at 100 to 600 micrograms daily in divided doses for the first two weeks, with a median maintenance dose around 450 micrograms daily. VIPoma dosing begins at 200 to 300 micrograms daily. The multiple-daily-injection burden is the primary reason most long-term patients are transitioned to the depot formulation.
Intramuscular depot (Sandostatin LAR). Once a patient demonstrates tolerance and response to the subcutaneous formulation, most clinicians transition to Sandostatin LAR, given as a single deep intramuscular gluteal injection every four weeks. For acromegaly, the initial LAR dose is typically 20 mg per month, adjusted based on biochemical response to 10 or 30 mg. For carcinoid syndrome, 20 mg monthly is standard. The depot formulation dramatically improves adherence and is the dominant form used in long-term management.
Oral capsule (Mycapssa). In 2020, the FDA approved Mycapssa (oral octreotide capsule) for long-term acromegaly maintenance in patients who have already responded to injectable somatostatin analogs. Peptides like octreotide are normally degraded in the GI tract before meaningful absorption occurs. Mycapssa overcomes this using transient permeation enhancer (TPE) technology, which temporarily increases small intestinal permeability to allow paracellular absorption. Clinical data confirm consistent biochemical normalization of IGF-1 and GH with a safety profile comparable to injectable formulations (PMID 37755395). The standard dose is 40 mg twice daily on an empty stomach. It is not appropriate for de novo treatment initiation and requires physician guidance for transition from injectables.
Side Effects and Gallstone Monitoring
The side-effect profile of octreotide is well-characterized across decades of clinical use. Knowing the main signals is important for anyone prescribed this drug, because some of them require active monitoring rather than passive symptom watching.
Gastrointestinal effects. These are the most common complaints and occur in the majority of patients. The prescribing information for octreotide acetate reports diarrhea, loose stools, nausea, and abdominal discomfort each in 34% to 61% of acromegalic patients (DailyMed NDA 019667). These symptoms are often most pronounced at the start of therapy and tend to diminish over the first few weeks. Fat malabsorption (steatorrhea) can also develop because octreotide suppresses pancreatic enzyme and bile acid secretion, which are necessary for fat digestion. New-onset steatorrhea, loose oily stools, or unexplained weight loss should prompt evaluation for pancreatic exocrine insufficiency.
Gallstones (cholelithiasis). This is the side effect that deserves the most attention because it is both common and often underestimated. Octreotide suppresses cholecystokinin, a hormone normally responsible for triggering gallbladder contraction after meals. Reduced gallbladder motility allows bile to become supersaturated and sludge or stones to form. The DailyMed prescribing label reports a 63% overall incidence of biliary tract abnormalities in clinical trials, including 27% gallstones, 24% biliary sludge without stones, and 12% biliary duct dilatation. In a prospective study of 44 patients receiving chronic octreotide for metastatic carcinoid or islet cell tumors, the overall incidence of cholelithiasis and sludge reached 52.3%, varying from 35.3% at lower doses to 66.6% at higher doses (PMID 9024721). Importantly, most of these stones are asymptomatic. In that same study, only 6.8% of patients required surgical intervention for symptomatic disease. The practical implication is that clinicians recommend baseline ultrasound before starting octreotide and periodic follow-up imaging, typically every 6 to 12 months, during long-term therapy. The finding of asymptomatic stones does not necessarily require stopping treatment, but it does require clinical judgment and ongoing monitoring.
Glucose metabolism. Octreotide's inhibition of both insulin and glucagon creates a complicated glucose picture. Hypoglycemia occurs in some patients (documented in 3% of acromegalics in trials) because the drug blunts the glucagon counter-regulatory response to falling glucose. Hyperglycemia occurs more often (16% of acromegalics) because insulin suppression outweighs the loss of glucagon. Patients with pre-existing diabetes need careful dose adjustment of their anti-diabetic medications, and blood glucose monitoring is standard practice at treatment initiation. Patients without diabetes should still have glucose assessed periodically.
Thyroid function. Octreotide suppresses TSH, and 12% of acromegalic patients developed biochemical hypothyroidism during treatment. Baseline thyroid function tests and periodic monitoring are standard.
Cardiac effects. Bradycardia developed in 25% of acromegalic patients in trials. Complete atrioventricular block has been reported with IV administration, so cardiac monitoring is standard when the drug is given intravenously.
Pregnancy. Data on octreotide use during human pregnancy are limited. Insufficient evidence exists to draw firm conclusions. Women who are pregnant or planning pregnancy should consult their physician before continuing or initiating octreotide.
The Bodybuilding Myth
Starting around the mid-2000s, a claim circulated in bodybuilding communities that octreotide could be used for "spot reduction" by suppressing GH or managing insulin dynamics to preferentially burn fat in targeted areas. The appeal is understandable: octreotide genuinely suppresses GH and affects insulin secretion, so it sounds like it might have body-composition implications. That is where the logic stops.
No clinical evidence supports octreotide for cosmetic body composition improvement, spot reduction, or physique enhancement. Systemic GH suppression in a healthy person does not produce cosmetic fat reduction; it more reliably causes insulin dysregulation, glucose abnormalities, gallstone formation, and thyroid suppression. No clinical trial has tested octreotide for these purposes, and the risk-benefit calculation that makes octreotide appropriate for a patient with acromegaly or metastatic carcinoid disease is entirely different from the one facing a healthy person seeking a physique advantage. Off-label use of octreotide for cosmetic purposes is without supporting trials and carries documented medical risks in the absence of any established benefit for that use.
For a broader look at which peptides fall into the legitimate FDA-approved category, see the FDA-approved peptides guide. For context on how bodybuilding peptide claims stack up against the evidence, see the peptides for bodybuilding overview.

Frequently Asked Questions
Is octreotide the same as Sandostatin? Yes. Sandostatin is Novartis's brand name for octreotide acetate injection; Sandostatin LAR is the long-acting depot form. Generic octreotide acetate is available from multiple manufacturers.
When was octreotide approved by the FDA? The original FDA approval for Sandostatin (octreotide acetate injection) was in 1988, making it one of the longer-tenured synthetic peptide drugs in active clinical use. Sandostatin LAR followed later as an additional formulation. Mycapssa (oral octreotide capsule) received FDA approval in 2020.
Does octreotide treat cancer? Octreotide treats symptoms caused by hormone-secreting neuroendocrine tumors, not the tumors themselves. The prescribing information is explicit that trials did not demonstrate improvements in tumor size or growth rate.
Can octreotide affect blood sugar in people who do not have diabetes? Yes. Octreotide suppresses both insulin and glucagon, which can cause glucose to swing in either direction. Trials documented both hypoglycemia and hyperglycemia in acromegalic patients without a prior diabetes diagnosis. This effect is real and warrants monitoring.
What happens if gallstones develop during octreotide treatment? Most octreotide-associated gallstones are asymptomatic and found on scheduled monitoring ultrasounds. Asymptomatic stones do not automatically require stopping treatment. Whether to continue, adjust, or stop octreotide when stones appear depends on symptoms, the severity of the underlying condition, and the overall risk-benefit assessment, all of which belong to the treating physician.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion
Octreotide is a well-established, FDA-approved synthetic peptide with a clear mechanistic rationale and three decades of clinical data behind it. For patients with acromegaly, carcinoid syndrome, or VIPoma, it addresses conditions that can cause serious harm, and the evidence supporting its use in those populations is substantial. The introduction of Mycapssa as an oral formulation in 2020 represents a meaningful advance for patients who would otherwise face indefinite injectable therapy.
The drug's side-effect profile is real and requires active management, not passive monitoring. Gallstone formation in over half of long-term patients is the highest-frequency serious concern, but glucose dysregulation, thyroid suppression, and cardiac effects all belong on the checklist during treatment initiation and follow-up.
What octreotide is not is a body-composition or wellness peptide. The circulating bodybuilding mythology about spot reduction or GH-modulation for physique purposes has no clinical trial evidence behind it, and it ignores a documented adverse-effect profile that makes off-label cosmetic use a straightforward unfavorable risk-benefit proposition.
If your physician has prescribed octreotide for an approved indication, the relevant next step is working with your endocrinologist on the monitoring protocol your specific formulation and dose require. If you encountered octreotide through a wellness or bodybuilding channel, the context above should reframe what you are reading about this drug.
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Octreotide is a prescription medication regulated by the FDA. All decisions regarding its use, dosing, and monitoring should be made by a qualified physician who has evaluated your individual health status. Do not start, stop, or adjust octreotide or any other prescription drug based on information found online.
