Before you decide
This article is general health information, not medical advice for your specific case. Tacrolimus is a narrow-therapeutic-index drug, and transplant care is highly individualized, so the people who matter most here are your transplant nephrologist and transplant pharmacist.
If you take tacrolimus (Prograf, Astagraf XL, Envarsus XR) or cyclosporine after a kidney, liver, heart, or other transplant, you are the highest-risk group for the magnesium problem described below. The same applies to some people taking these drugs for severe autoimmune disease.
The short version: low magnesium on tacrolimus is expected and usually manageable. What follows explains why it happens, how often, what symptoms to watch, and why repletion belongs with your team rather than the supplement aisle. For the bigger picture of how prescriptions and supplements collide, our guide to drug and supplement interactions is a good starting point.
What the interaction actually is
Tacrolimus and cyclosporine belong to a class called calcineurin inhibitors. Their main job is to quiet the immune system so it does not attack a transplanted organ. A predictable side effect is that they make the kidneys waste magnesium.
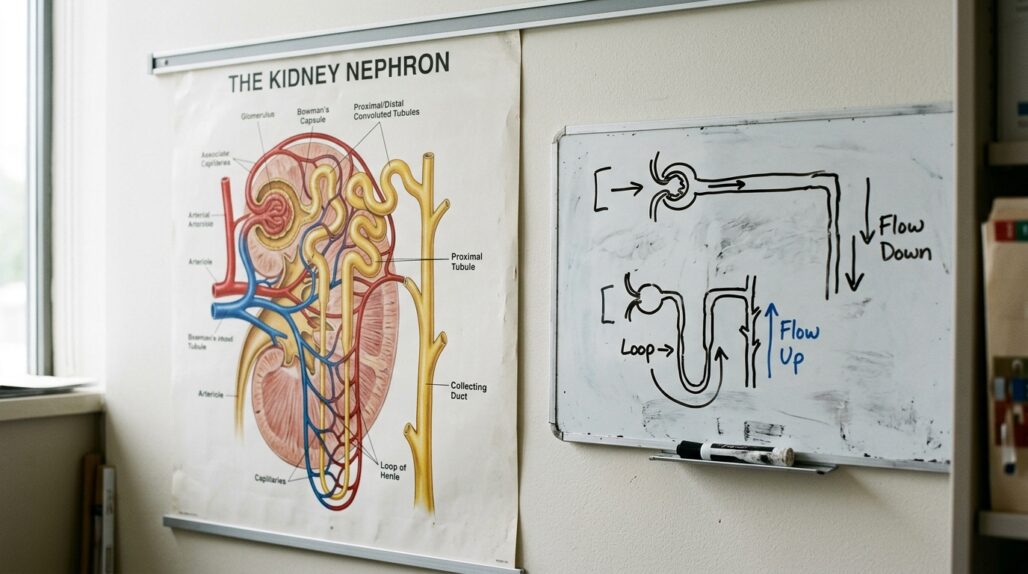
The mechanism is now well mapped. In the distal convoluted tubule – the part of the kidney that fine-tunes how much magnesium you keep – reabsorption runs through a channel called TRPM6. Calcineurin inhibitors lower how much TRPM6 the kidney makes, so magnesium that should be reclaimed slips out into the urine instead. A 2018 review in Frontiers in Medicine on electrolyte disorders in transplant recipients describes TRPM6 as the main site for active magnesium reabsorption, and notes that calcineurin inhibitors decrease its expression.
The original observation that tacrolimus reduces TRPM6 traces back to work by Nijenhuis and colleagues. A later mouse study published in Physiological Reports (Gratreak et al., 2020) pinned the cause more precisely: animals engineered to lack FKBP12, the protein tacrolimus needs to block calcineurin, were completely protected from the magnesium loss. That points the finger at calcineurin inhibition itself, not some unrelated drug toxicity.
So this is not a vague "supplement clash." It is a direct, dose-related effect of the drug on a specific kidney channel.
How common it is, and how big the effect
Low magnesium is one of the most frequent electrolyte issues after transplant. A 2025 analysis in the International Journal of Molecular Sciences looked at kidney transplant recipients and found hypomagnesemia in about 50.7% of them – the single most common electrolyte disorder in the group.
Tacrolimus stands out as a driver. In that same analysis, tacrolimus use was an independent risk factor for low magnesium, with an odds ratio of about 2.91. Patients on tacrolimus ran lower average magnesium than those on mTOR inhibitors, and higher tacrolimus blood levels tracked with more magnesium in the urine – a dose-dependent pattern.
The effect tends to be strongest early after transplant, when tacrolimus levels are deliberately kept higher, and it often eases somewhat as target levels come down over time. It is generally worse with tacrolimus than with cyclosporine.
There is also a worrisome downstream signal. Researchers have linked post-transplant hypomagnesemia to new-onset diabetes after transplant, which is part of why teams take it seriously rather than shrugging at a slightly low number.
Symptoms worth flagging
Mild low magnesium often causes nothing you would notice, which is exactly why it is usually caught on routine bloodwork rather than from how you feel. When magnesium drops further, symptoms can show up.
Watch for and report:
- Muscle cramps, spasms, or twitching, especially in the legs or around the eyes
- Heart palpitations or an irregular heartbeat – magnesium loss can drag potassium and calcium down with it
- Persistent fatigue or weakness that is not explained by your usual recovery
- Numbness, tingling, or in severe cases, confusion or seizures
These are not reasons to panic, but they are reasons to call your team rather than wait for the next scheduled visit. A fast or irregular heartbeat with cramping deserves a same-day call, and chest pain, fainting, or a seizure is a reason to seek emergency care.

The repletion approach – and why it is your team's call
Here is where many people want to take charge and buy a magnesium supplement. With tacrolimus, that instinct can backfire, and the reasons are practical rather than dramatic.
First, magnesium repletion in transplant patients is often tiered by severity. The Frontiers in Medicine review suggests reserving supplementation for moderate (below roughly 1.5 mg/dL) and severe (below roughly 1.2 mg/dL) hypomagnesemia, and using intravenous magnesium first for severe or symptomatic cases, followed by oral dosing. That triage needs a lab value and a clinician, not a guess.
Second, oral magnesium does not always work well in this setting. The 2025 analysis found that supplemented patients did not reliably reach higher levels – partly because some forms are poorly absorbed and partly because the kidney keeps wasting what you take in. Throwing more pills at it without monitoring can mean a lot of stomach upset for little gain.
Third, the dose-limiting side effect of oral magnesium is diarrhea. The NIH Office of Dietary Supplements magnesium fact sheet sets the upper limit for supplemental magnesium at 350 mg per day for adults, with diarrhea as the limiting factor, and notes that oxide and other poorly soluble salts are common culprits. The more bioavailable, gentler forms tend to be the chelated and well-dissolving ones.
The table below summarizes how the common forms differ. Treat it as background for a conversation with your pharmacist, not a shopping list.
| Magnesium form | Relative absorption | GI tolerance | Practical note |
|---|---|---|---|
| Glycinate (bisglycinate) | Higher | Usually gentle | Often preferred when stomach upset is the problem |
| Citrate | Higher | Can loosen stools | Effective but more likely to cause diarrhea at higher doses |
| Oxide | Lower | Frequent diarrhea | Cheap and common, but poorly absorbed per the NIH fact sheet |
| Intravenous | Complete | Not applicable | Hospital or clinic only, reserved for severe or symptomatic lows |
If your team does prescribe oral magnesium, a few timing habits help. Splitting the daily amount into smaller doses across the day is gentler on the gut and tends to be absorbed better than one large dose. Taking it with food can ease nausea. And because magnesium can bind some other drugs, your pharmacist may ask you to space it apart from certain medications – another reason to map it out with them rather than improvise. For a broader look at how the salts compare, see our explainer on magnesium forms and bioavailability compared and our wider complete guide to magnesium.
The grapefruit warning that matters more than any supplement
While magnesium is the headline here, there is a food interaction that is genuinely dangerous with tacrolimus, and it is worth more of your attention than any pill.
Avoid grapefruit and grapefruit juice entirely. Tacrolimus is broken down by an enzyme called CYP3A4, and grapefruit blocks that enzyme. The result is that tacrolimus piles up in your blood. The FDA's consumer update on grapefruit and medicines explains that for affected drugs the juice lets more of the drug enter the bloodstream, raising the risk of side effects.
With a narrow-therapeutic-index drug like tacrolimus, that spike can mean kidney injury, tremor, and a higher chance of toxicity. The effect lingers for days because grapefruit's compounds disable the enzyme rather than just competing with it. Seville oranges, pomelos, and tangelos can do the same thing, so steer clear of those too.
This is the one diet-drug rule on this page that is close to absolute. Magnesium is something your team adjusts; grapefruit is something you simply skip.

When to involve your clinician
For people on tacrolimus, the honest answer is that magnesium decisions should run through your team from the start. Concretely, reach out when:
- Your routine labs show low magnesium and you are unsure whether you should be supplementing
- You notice cramps, palpitations, twitching, or unusual weakness
- You want to add any magnesium product, including a multivitamin or a sleep blend that contains it
- You are also taking a diuretic, a proton pump inhibitor, or other drugs that can lower magnesium further
If you juggle several prescriptions and supplements, it helps to keep one current list you can hand to a pharmacist. The free app StackMyMed lets you log your stack and flag possible interactions to raise at your next visit. It is a prompt for a real conversation, not a substitute for your transplant team's judgment.
Because tacrolimus sits alongside other immunosuppressants and the rules differ by organ and kidney function, it is also worth reading our guidance on kidney-friendly vitamins and medications and our overview of drug and supplement conflicts in autoimmune disease.
FAQ
Does tacrolimus really cause low magnesium? Yes. Tacrolimus and other calcineurin inhibitors lower the kidney’s TRPM6 channel, so more magnesium is lost in urine. Studies suggest roughly half of kidney transplant recipients run low, and tacrolimus is an independent risk factor.
Can I just buy a magnesium supplement to fix it? Not on your own. Repletion in transplant patients is often dosed by lab value and severity, oral magnesium is not always well absorbed in this setting, and your team needs to weigh kidney function and other medications first.
Which magnesium form is best if my team prescribes one? Glycinate and citrate are generally better absorbed and gentler than oxide, which often causes diarrhea. The NIH notes diarrhea is the dose-limiting side effect, which is why the upper limit for supplemental magnesium is 350 mg a day for adults. Let your pharmacist match the form and dose to you.
Why does low magnesium matter beyond cramps? Besides muscle and heart symptoms, research has linked post-transplant hypomagnesemia to new-onset diabetes after transplant, so teams monitor it rather than ignoring a mildly low number.
Is grapefruit really that dangerous with tacrolimus? Yes, and it deserves more caution than any supplement. Grapefruit blocks the CYP3A4 enzyme that clears tacrolimus, which can raise drug levels and the risk of kidney problems and toxicity for days. Avoid grapefruit, Seville oranges, pomelos, and tangelos.
How often should my magnesium be checked? That is set by your transplant team and usually built into your routine labs, more often early after transplant when tacrolimus levels are higher. Ask what your target range is and when you are next due.
Conclusion: a normal, manageable side effect – with one hard rule
Low magnesium on tacrolimus is common, well understood, and usually handled with monitoring and measured repletion. The mechanism is a real, dose-related effect on a kidney channel, not a fluke, so seeing it on your labs does not mean something has gone wrong.
The practical takeaway is simple. Let your transplant team check and replete your magnesium rather than self-dosing, report cramps or palpitations promptly, and treat the grapefruit warning as non-negotiable. Bring a current list of everything you take to your next appointment and let your pharmacist sort the timing.
This article is for general education and does not replace personalized advice from your transplant team or pharmacist. Tacrolimus has a narrow safety margin, so never start, stop, or change a medication or supplement without your clinician.
Reviewed by the UsefulVitamins Editorial Team.
