Thymosin alpha-1 is one of the more genuinely interesting peptides in this series — approved in more than 35 countries for hepatitis B and hepatitis C, backed by two decades of peer-reviewed research across multiple independent groups, and yet formally unavailable in the United States. Since 2023, compounding pharmacies operating under Section 503A of the Federal Food, Drug, and Cosmetic Act have been explicitly prohibited from producing it for human use. The honest answer to "should I get it from a grey-market vendor or a US compounding pharmacy" is not a qualified maybe. It is a clear no, and the reasoning is more nuanced than most wellness influencers suggest. This article covers what thymosin alpha-1 actually is, what the clinical evidence supports, where the US regulatory situation stands, and what anyone considering this peptide needs to know.
If you are new to peptide biology, start with our introduction to what peptides are and how they work. If you want a broader view of peptide safety, our guide to peptide safety covers the framework for evaluating compounds in this category.
What Thymosin Alpha-1 Actually Is
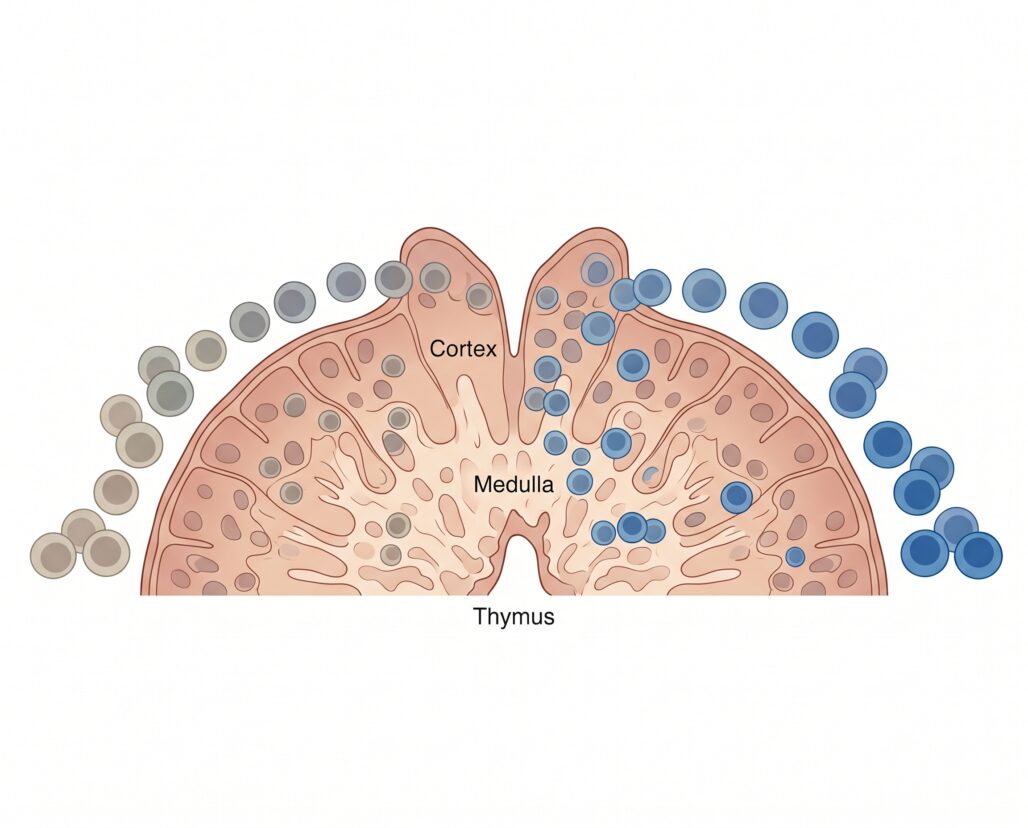
Thymosin alpha-1 (abbreviated Tα1) is a synthetic 28-amino-acid peptide derived from prothymosin alpha, a protein that occurs naturally in the thymus gland. The thymus is a small organ in the upper chest where immature T-cells — originating in bone marrow — complete their maturation and acquire the capacity to recognize specific threats. The natural peptide was first isolated from bovine thymic tissue by Allan Goldstein and colleagues at George Washington University in the 1970s; the synthetic version replicates the same structure at consistent purity.
At 28 amino acids, Tα1 is stable enough for subcutaneous injection, which is the route used in all clinical trials. Oral bioavailability is essentially zero: proteases in the gastrointestinal tract degrade the peptide before it reaches systemic circulation. Any product marketing oral thymosin alpha-1 is selling something that will not survive the stomach intact.
One clarification worth making explicitly: thymosin alpha-1 and thymosin beta-4 (sold as TB-500 in grey-market channels) are different peptides with different sequences, different molecular targets, and different clinical profiles. They share the word "thymosin" because both were originally isolated from thymic extracts — and that is where the similarity ends. Vendors and online communities sometimes conflate the two. If you are being sold "thymosin" without a clear alpha-1 or beta-4 designation, treat that as a red flag.
The International Approval Landscape: Zadaxin in 35+ Countries
The commercial form of synthetic thymosin alpha-1, branded as Zadaxin by SciClone Pharmaceuticals, has been approved in more than 35 countries — primarily across Asia, the Middle East, Latin America, and parts of Europe. The primary approved indications are chronic hepatitis B, chronic hepatitis C (in combination with interferon-based regimens), and immune restoration in immunocompromised patients. China includes Zadaxin in national hepatitis B treatment guidelines; Italy approved it as an adjunct for elderly influenza vaccination; several other markets have authorized it in sepsis and chemotherapy-associated immune suppression.
The standard dosing regimen is 1.6 mg subcutaneously twice per week, for 6 to 12 months depending on the indication. This is a biologically active injectable peptide requiring medical supervision, sterile injection technique, and regular laboratory monitoring — not a consumer supplement.
The breadth of international approval is meaningful: it confirms a recognized mechanism and an established clinical profile. It does not mean the FDA has reviewed and accepted that evidence. In the case of thymosin alpha-1, the FDA has not.
The US Regulatory Reality: Orphan Designation Without Approval, and a 503A Ban
The FDA granted thymosin alpha-1 orphan drug designation for hepatocellular carcinoma — a development incentive that confers extended exclusivity periods, tax credits for trial costs, and waived application fees. Orphan designation does not constitute approval and does not grant the right to market or sell a compound. No marketing application for thymosin alpha-1 has been approved by the FDA. There is no US-approved brand of Zadaxin and no FDA-cleared indication for any disease in any population in the United States.
The compounding pharmacy question became unambiguous in 2023. Under Section 503A of the Federal Food, Drug, and Cosmetic Act, compounding pharmacies may use bulk drug substances that the FDA has placed on an approved list (Category 1), while Category 2 substances are those the FDA has evaluated and determined should NOT be included — meaning 503A compounding pharmacies cannot legally use them to prepare human drugs. Thymosin alpha-1 was placed on the Category 2 interim list. A US physician prescription filled by a 503A compounding pharmacy is not a legally compliant route to this drug. Vendors selling "research grade" thymosin alpha-1 online are operating entirely outside the regulatory framework — the FDA does not certify, inspect, or endorse those products.
If you are currently using thymosin alpha-1 sourced from a US compounding pharmacy and were told it was legal, the regulatory landscape changed in 2023. Verify current status with the prescribing provider.
How Thymosin Alpha-1 Works: T-Cell Maturation and Immune Modulation
Understanding why thymosin alpha-1 has been studied for such a range of immune-related conditions requires understanding what the thymus does and what happens when its function declines.
The thymus is not simply a T-cell factory. It is a T-cell quality control system. Immature T-cells that migrate from bone marrow enter the thymus, where a complex biochemical environment trains them to distinguish self from non-self. Cells that react too weakly to antigenic signals are eliminated as useless; cells that react too aggressively to the body's own tissues are eliminated as dangerous. The cells that survive this dual selection process — positive and negative selection — leave the thymus as mature, antigen-specific T-cells capable of targeted immune responses.
The thymus begins to shrink after puberty in a process called thymic involution. By age 60, it has typically replaced most of its functional tissue with fat. This progressive decline is one of the reasons immune response quality decreases with age and why older adults respond less robustly to vaccines.
Thymosin alpha-1 appears to mimic signals the thymus generates to promote T-cell maturation. Documented effects include enhancing differentiation of immature T-cell precursors into functional T helper (CD4+) and cytotoxic T (CD8+) cells, boosting natural killer (NK) cell activity, and stimulating dendritic cells to present antigens more effectively — producing a measurable enhancement of cell-mediated immunity across multiple in vitro and in vivo models.
A 2015 review published in Expert Opinion on Biological Therapy (PMID 25640173) described the mechanism as correcting deficits in immunocompromised patients rather than indiscriminately amplifying immune activity. The available evidence does not suggest Tα1 functions as a blanket stimulant in immunologically healthy individuals. That distinction matters for understanding both the therapeutic rationale and the safety profile.
Clinical Evidence: Hepatitis, Elderly Vaccine Response, and Sepsis
The strongest clinical evidence for thymosin alpha-1 sits in two areas: chronic hepatitis B treatment and vaccine response enhancement in immunocompromised populations. The hepatitis C and sepsis data are more mixed.
Chronic Hepatitis B
A meta-analysis in the World Journal of Gastroenterology (PMID 18078676) examined four randomized controlled trials in 199 patients with chronic hepatitis B. At end of treatment, interferon-alpha showed higher virological and biochemical response rates. At 6-month follow-up, the picture reversed substantially: virological response favored Tα1 with an odds ratio of 3.71 (95% CI: 2.05 to 6.71), biochemical response OR 3.12 (95% CI: 1.74 to 5.62), and complete response OR 2.69 (95% CI: 1.47 to 4.91).
The interpretation is that Tα1 achieves its benefit differently than interferon-alpha: rather than suppressing viral replication directly, it rebuilds the immune capacity to sustain control after treatment ends. That delayed but durable benefit profile is exactly what the mechanism would predict.
Combination therapy studies showed additional benefit. A comprehensive review published in Drugs (PMID 11381492) reported that combining Tα1 with interferon alfa-2b for hepatitis C achieved viral RNA clearance in 65% of patients compared to 29% in the interferon-alone group, and normalized liver enzyme levels in 71% versus 35%. These results are notable, though the hepatitis C landscape has been transformed by direct-acting antivirals since this literature was generated, and the clinical relevance for hepatitis C specifically has diminished.
Vaccine Response in Immunocompromised Patients
A 2012 pilot study by Carraro and colleagues (PMID 22178096) examined whether thymosin alpha-1 could enhance the immunogenicity of a pandemic H1N1 influenza vaccine in hemodialysis patients. Dialysis patients mount characteristically poor vaccine responses because chronic kidney disease impairs immune function and erodes thymic T-cell output. The combination of Tα1 with an adjuvanted H1N1 vaccine produced seroconversion by day 21 and fully satisfied regulatory criteria for pandemic vaccine licensing in elderly subjects, while the vaccine-alone group showed weaker responses. No adverse events attributable to Tα1 were observed, and no impacts on blood parameters or cardiac function were detected.
This is a small pilot study, and it should be read as hypothesis-generating rather than definitive. But it illustrates the clinical niche where thymosin alpha-1's mechanism is most plausible: populations with blunted immune function who need to mount a stronger and more sustained response than their depleted T-cell capacity would otherwise allow.
Sepsis
Several Asian clinical guidelines have included Tα1 as an adjunct in sepsis management, based on the rationale that sepsis frequently induces immune paralysis — a state where T-cells become exhausted and unresponsive even as the infection continues. The clinical evidence here is suggestive but inconsistent, and no large randomized trial has established Tα1 as a standard-of-care adjunct for sepsis in the United States or Western Europe. Any claim that thymosin alpha-1 has "proven sepsis benefit" is running ahead of the data as it stands.
Safety Profile: What the Clinical Record Shows
The safety record of thymosin alpha-1 across more than two decades of clinical use in approved markets is notably clean. The most commonly reported adverse effect is transient local irritation at the injection site. Across the clinical trials summarized in pharmacological evaluations (PMID 11381492), systemic adverse events were rare. The drug does not suppress bone marrow function, does not carry the flu-like symptoms associated with interferon therapy, and has not been associated with the autoimmune complications seen with some immunostimulatory agents. Serum half-life is approximately 2 hours, with clearance within 24 hours post-injection.
Important gaps remain. There is insufficient published data on thymosin alpha-1 in pregnancy and lactation — women who are pregnant or nursing should not use this compound. Whether Tα1 is safe in immunologically healthy individuals has not been studied systematically. The assumption that immune modulation is always beneficial is not supported by the pharmacological evidence.
That clean safety record applies to pharmaceutical-grade Zadaxin manufactured under controlled conditions, administered in known doses, and monitored with regular laboratory follow-up. The same record cannot be assumed for grey-market products of unknown purity and unknown peptide sequence.
Who Thymosin Alpha-1 Is Actually For
The populations with the most meaningful clinical rationale are: patients with chronic hepatitis B inadequately controlled on antiviral therapy alone who can access Zadaxin in a country where it is approved; and immunocompromised patients — those on chemotherapy, dialysis, HIV treatment, or long-term immunosuppression — who are poor vaccine responders and whose physicians are considering supervised adjunct strategies.
In the United States, there is no legal path to pharmaceutical-grade Zadaxin. Compounding pharmacies cannot produce it under 503A as of 2023. Grey-market vendors are selling an unapproved drug substance of unknown quality outside the regulatory framework. The evidence base, while compelling for specific clinical indications, was not built in contexts that resemble a healthy adult seeking immune enhancement.
Do not self-source thymosin alpha-1 from grey-market vendors. If you have a specific clinical situation — a hepatitis diagnosis, an immune deficiency, documented poor vaccine response — discuss the international evidence with a hepatologist or infectious disease specialist. They can advise whether accessing Zadaxin in a country where it is approved makes clinical sense, or whether FDA-approved alternatives address the same underlying problem.
For the broader context of immune modulation, our articles on peptides for autoimmune conditions and peptides for inflammation cover how evidence in this category is evaluated.
Frequently Asked Questions
Is thymosin alpha-1 the same as TB-500 or thymosin beta-4? No. Both were originally isolated from thymic tissue, which is why they share the "thymosin" prefix, but the amino acid sequences, molecular targets, and documented effects are entirely different. Grey-market vendors sometimes conflate or mislabel them. If you are being sold "thymosin" without a clear alpha-1 or beta-4 designation, that is a red flag about the information quality you are receiving.
Is Zadaxin available in the US by prescription? No. Zadaxin has not been FDA-approved. As of the Category 2 interim designation in 2023, no 503A compounding pharmacy can legally fill a US prescription for thymosin alpha-1. Any vendor claiming otherwise is operating outside the regulatory framework.
Does the FDA orphan drug designation mean thymosin alpha-1 is partly approved? No. Orphan designation is a development incentive — extended exclusivity periods, tax credits, waived fees — not an approval. It does not authorize marketing or clinical use.
What should I do if I have chronic hepatitis B and want to explore thymosin alpha-1? Speak with a hepatologist or infectious disease specialist. They can review your treatment regimen and discuss whether accessing Zadaxin in a country where it is approved is clinically warranted. Do not self-source.
Is thymosin alpha-1 safe if I am immunologically healthy? The clinical evidence was built in immunocompromised populations, not healthy adults. Whether the safety profile translates to healthy individuals using it for general immune enhancement has not been studied. The assumption that more immune stimulation is always beneficial is not supported by the pharmacological rationale.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion
Thymosin alpha-1 is not a fringe compound with no legitimate scientific basis. It has more than 35 country approvals, two decades of clinical research, multiple independent research groups, and a mechanism that is well-understood in the context of thymic biology and T-cell maturation. The evidence for chronic hepatitis B is among the more compelling clinical records in this peptide series, particularly the durable post-treatment benefit demonstrated in the meta-analysis comparing Tα1 with interferon-alpha.
What the evidence does not support is the wellness community's reframing of this drug as a general immune booster available through grey-market vendors. The US regulatory status is unambiguous: not FDA-approved, not legally compoundable under 503A as of 2023, and not available through any compliant US supply chain. The grey-market products sold online carry the full range of risks that accompany unverified peptide sources — unknown purity, variable concentration, potential contamination, and no post-market surveillance.
If your interest in thymosin alpha-1 is driven by a genuine clinical need — chronic hepatitis, documented immune compromise, poor vaccine response — that interest deserves a real conversation with a hepatologist or infectious disease specialist who can advise within a supervised clinical framework. If your interest is driven by wellness optimization in the absence of a specific deficiency, the evidence base does not support the risk of obtaining an unapproved compound from an unregulated source.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Thymosin alpha-1 (Zadaxin) is approved for hepatitis B, hepatitis C, and certain adjunct indications in more than 35 countries but is NOT FDA-approved in the United States and has been placed on the FDA Category 2 503A bulk drug substance interim list, meaning US compounding pharmacies cannot legally compound it for human use. Do not self-source thymosin alpha-1 from grey-market vendors. Patients with hepatitis, immune deficiency, or related conditions should consult a hepatologist or infectious disease specialist. International approval does not equal US approval. There is insufficient data on thymosin alpha-1 in pregnancy and lactation. Always seek the guidance of a qualified healthcare professional before beginning, modifying, or discontinuing any medical treatment.
