If you are a man over 40 and you have spent any time on fitness forums or wellness podcasts, someone has probably told you that peptide therapy will restore your growth hormone levels, fix your recovery, and give you the body composition of your 30-year-old self. Some of that marketing is attached to real biochemistry. Most of it is attached to grey-market compounds with no adequate human safety record and no FDA approval as dietary supplements. The honest answer is narrower and more useful: one category — oral collagen peptides — has genuine clinical support for joint recovery and muscle maintenance in middle-aged men; the injectable GHRP compounds most frequently marketed for "rejuvenation" are research chemicals, not approved therapies; and testosterone is not a peptide at all, no matter how many supplement brands imply otherwise.
Summary / Quick Answer: Do Peptides Help Men Over 40?
The short answer: oral collagen peptides have the best evidence for joint recovery, exercise-related soreness, and lean mass support in this age group when combined with resistance training. Growth hormone-releasing peptides (GHRPs) such as CJC-1295, ipamorelin, and MK-677 are NOT FDA-approved as dietary supplements and are sold as research chemicals not intended for human use. Testosterone replacement therapy is a separate, physician-supervised medical intervention — and testosterone is a steroid hormone, not a peptide.
Best for:
- Men 40-65 with joint discomfort, slow connective tissue recovery, or early signs of sarcopenia
- Anyone looking for a low-risk complement to an existing resistance training and protein intake routine
- Men researching what the science actually says before spending money on supplements marketed for "male rejuvenation"
Not ideal for:
- Replacing physician evaluation if symptoms of hypogonadism are present — low libido, fatigue, and significant body composition changes deserve lab work, not supplements
- Anyone expecting GHRPs to deliver the body composition of exogenous growth hormone without the regulatory and safety profile that comes with it
- Men drawn in by peptide clinics offering injectable protocols outside a documented clinical indication
What to look for:
- Hydrolyzed collagen peptides: 10-15 g/day, ideally taken 60 minutes before resistance training sessions with a vitamin C source
- Minimum 12 weeks of consistent use alongside progressive resistance training before evaluating results
- Products with published brand-specific RCT data rather than generic collagen marketing claims
Decision shortcut: If you are experiencing symptoms that might indicate low testosterone — consistent fatigue, reduced libido, loss of muscle mass despite training — get a morning serum testosterone panel before spending anything on supplements. No peptide supplement raises testosterone meaningfully, and several GHRP compounds interfere with insulin signaling, which is the opposite of what most men over 40 need.
What Actually Changes After 40: The Physiology Behind the Marketing
The changes men notice in their 40s are real, well-documented, and give supplement marketers a legitimate hook. Understanding the actual biology makes it easier to separate the reasonable interventions from the wishful ones.
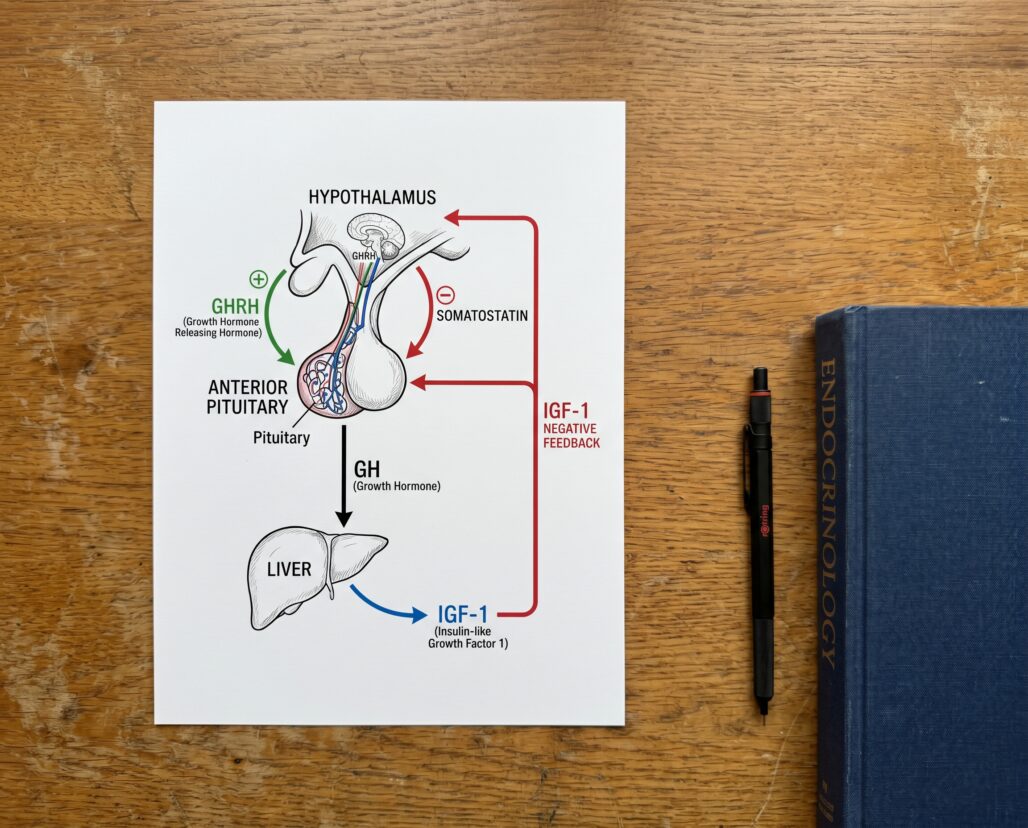
Growth hormone output declines by roughly 15% per decade after the third decade of life. Peak GH secretion drops from approximately 150 mcg/kg/day at puberty to around 25 mcg/kg/day by age 55 (NBK279163). The primary driver is not a pituitary failure but a reduction in nocturnal GH pulse amplitude — the large overnight releases that govern tissue repair and body composition. IGF-1 declines in parallel, mainly because less GH is secreted rather than because tissues have become resistant.
Testosterone declines more slowly than most men expect. Total serum testosterone falls at approximately 0.4% per year in men aged 40-70, while free testosterone — the biologically active fraction — drops at a steeper 1.3% per year due to rising sex-hormone-binding globulin (PMID 35393533). This is real but gradual. A 2012 review (PMID 22505891) found that the symptoms most reliably linked to biochemically confirmed low testosterone are three sexual ones: reduced morning erections, reduced frequency of sexual thoughts, and erectile dysfunction — not general fatigue or muscle loss, which have many other causes.
Connective tissue and muscle recovery genuinely slow down. Collagen synthesis in cartilage, tendons, and ligaments decreases with age, and slower extracellular matrix turnover means joint wear accumulates faster than it is repaired. This is the domain where collagen peptides, combined with mechanical loading from exercise, have the most coherent mechanism and the most replicable evidence.
The "Peptides for Men's Rejuvenation" Marketing Pipeline
The supplement and "peptide clinic" industries have built a substantial market around the idea that GHRPs can reverse the GH decline of aging in a safe, legal, and accessible way. The compounds most frequently marketed include CJC-1295 (a GHRH analogue), ipamorelin (a selective GHRP), and MK-677 (ibutamoren, an oral ghrelin mimetic).
None of these are FDA-approved as dietary supplements or as prescription medications for age-related GH decline. CJC-1295 and ipamorelin are listed on the World Anti-Doping Agency's prohibited list under Section S2 (peptide hormones and releasing factors). MK-677 was investigated by Merck and later Novo Nordisk as a potential treatment for muscle wasting and hip fracture recovery; those programs did not result in an approved drug. When these compounds appear on websites shipping to consumers, they are sold under the legal fiction of "research use only, not for human consumption" — a label that does not change what buyers are actually doing with them.
The real question is not whether these compounds raise IGF-1 — some of them clearly do in controlled settings. The real question is whether that IGF-1 elevation translates into meaningful, safe functional outcomes in healthy aging men, and the evidence there is substantially weaker than the marketing suggests.
GHRPs: What the Research Actually Shows
The published human data on GHRPs is more limited than the grey-market enthusiasm implies, and the functional outcome picture is inconsistent.
CJC-1295 does activate the GH/IGF-1 axis and produce measurable IGF-1 elevation in healthy adults (PMID 19386527). A dose-ranging study found that single injections produced sustained GH secretion for six days (PMID 16352683). The IGF-1 elevation is pharmacologically real. The problem is what comes next.
A review published in the journal Translational Andrology and Urology (PMC7108996) examined the body of human data on five GHS compounds — sermorelin, GHRP-2, GHRP-6, MK-677, and ipamorelin — in the context of hypogonadal and aging males. The authors found that ibutamoren (MK-677) at 25 mg/day increased IGF-1 by 55% at two weeks and 88% at four weeks, reaching levels normal for young adults. Fat-free mass increased by approximately 3 kg over eight weeks in one study. But the fat loss data was inconsistent, with some trials showing no change in total body fat despite the lean mass gains. More importantly, the review noted explicitly "a paucity of data examining the clinical effects of these compounds currently limits our understanding of GHS' role in the treatment of men with hypogonadism," and called for larger, longitudinal studies before clinical adoption.
MK-677 is also notable for its safety caveats: it elevates fasting glucose and insulin levels, a meaningful concern for men over 40 who are already at increased metabolic risk. Ipamorelin, described in an early characterization study (PMID 9849822) as the first selective GHRP, shows a more favorable cortisol and prolactin profile than older GHRPs, which is why it is frequently pitched as a "cleaner" option. But the human functional outcome data in aging men is still sparse, and its regulatory status remains the same: not approved for human therapeutic use.
Actionable takeaway: IGF-1 elevation is a lab finding, not a clinical outcome. No GHRP has demonstrated consistent improvements in strength, functional capacity, or quality of life in adequately powered human trials of middle-aged men. The compounds carry real safety signals — glucose dysregulation, potential cardiovascular effects from fluid retention, and unknown long-term risks — alongside a regulatory status that places them outside legitimate medical use for aging-related GH decline.
Testosterone Is Not a Peptide: The Clarification That Matters
This section exists because the peptide and "hormone optimization" marketing worlds frequently conflate two separate things, and the confusion is not accidental.
Testosterone is a steroid hormone synthesized from cholesterol in the Leydig cells of the testes, not assembled from amino acid chains. It is not a peptide. Testosterone replacement therapy (TRT) — the clinical intervention for documented hypogonadism — involves exogenous testosterone in injections, gels, or patches, not peptides.
Legitimate TRT is a physician-supervised treatment for men with documented low testosterone (typically total T below 300 ng/dL on two morning measurements) plus clinical symptoms. It is legitimate, is prescribed under FDA-approved indications, and has a substantial evidence base. A 2012 review (PMID 22505891) summarized that TRT in hypogonadal men improves sexual function, mood, and lean body mass, with a safety profile that is well-characterized when properly managed.
The tradeoff is that TRT suppresses endogenous testosterone production, requires ongoing monitoring, and is not appropriate for men who want to have children. It is also not appropriate for men with normal or borderline testosterone who simply feel tired — fatigue has too many other causes to attribute to testosterone in the absence of lab confirmation.
Actionable takeaway: If a clinic is selling you a "peptide protocol for testosterone optimization" that does not involve checking your actual testosterone level first, that is a red flag, not a service. The peptide compounds most associated with testosterone-adjacent marketing — such as kisspeptin analogues or GnRH peptides — are not approved for this use outside of specific research contexts, and none are available as dietary supplements.
Where Collagen Peptides Actually Fit for Men Over 40
Oral collagen peptides occupy a different position from GHRPs: they have genuine RCT data, a long safety record at common doses, and a mechanism that makes physiological sense for the specific problems aging men most commonly face — joint discomfort and slow connective tissue recovery.
A 2021 systematic review in Amino Acids (PMC8521576) covered 15 randomized controlled trials on collagen peptide supplementation across body composition, collagen synthesis, and recovery outcomes. The most striking data came from elderly sarcopenic men (average age 72 years) who took 15 g/day of collagen peptides alongside a 12-week resistance training program and gained 4.2 kg of fat-free mass compared to 2.9 kg in the placebo plus training group. Fat mass fell 5.4 kg versus 3.5 kg in controls. The review also noted that 5-15 g/day combined with exercise consistently improved joint pain markers across multiple studies.
A 2023 trial (PMID 37133292) specifically in healthy middle-aged males found that dietary collagen peptides significantly reduced exercise-induced muscle soreness in a randomized, double-blind crossover design. The mechanism proposed is that hydrolyzed collagen provides glycine, proline, and hydroxyproline — amino acids concentrated in connective tissue — that are not adequately supplied by whey or casein at standard doses.
A separate 2023 trial (PMID 37551682) found that collagen peptide supplementation improved function, pain scores, and both physical and mental outcomes in active adults, with effect sizes that held across different ages within the study population.
The important caveat is what collagen peptides do not do: they are not a muscle protein synthesis driver in the way whey protein is. The systematic review noted that whey produces substantially higher rates of myofibrillar protein synthesis than collagen gram-for-gram, because collagen lacks tryptophan and contains lower leucine concentrations. The use case for collagen is joints, tendons, and connective tissue — not replacing high-quality dietary protein for hypertrophy.
Actionable takeaway: Men over 40 who train regularly and deal with joint soreness or slow tendon recovery have a legitimate, evidence-backed reason to use hydrolyzed collagen peptides (10-15 g/day, taken 60 minutes before training sessions alongside vitamin C). This is not a replacement for adequate total protein intake or progressive resistance training — it is a targeted addition to both.
The Actual Evidence Base: Sleep and Resistance Training
The GH and testosterone marketing implicitly competes with two interventions that have far better evidence and zero regulatory concerns: consistent resistance training and adequate sleep.
Sleep architecture in men shifts after 40, with reductions in slow-wave (N3) sleep — the phase most associated with pulsatile GH release. The NCBI chapter on GH and aging (NBK279163) notes that the primary mechanism of somatopause is reduced nocturnal GH pulse amplitude, the same pulses most dependent on N3 sleep quality. Sleep debt increases cortisol and blunts both GH and testosterone secretion.
Resistance training stimulates GH secretion, though the peak response diminishes with age: 14.9 mcg/L in young subjects versus 2.44 mcg/L in elderly subjects in one controlled measurement (PMID 1639942). Critically, the functional benefits of resistance training in aging men appear largely independent of that GH response. Strength, bone density, insulin sensitivity, and cardiovascular risk markers all improve through mechanisms that do not require a young man's GH pulse amplitude.
A six-month resistance training program improved sleep quality by 38% in older adults alongside strength gains (PMC3887339). Better sleep drives better GH pulses, which supports tissue repair — a reinforcing loop that costs nothing.
Actionable takeaway: If you are a man over 40 sleeping less than seven hours per night and not yet doing structured resistance training three or more days per week, those two changes will do more for your GH output, body composition, and recovery than any GHRP compound could — without the safety unknowns, the cost, or the legal ambiguity.

FAQ
Do peptide supplements raise testosterone? No. No over-the-counter peptide supplement raises testosterone meaningfully. Compounds affecting the hypothalamic-pituitary-gonadal axis (such as kisspeptin analogues) are investigational, not approved, and not sold as dietary supplements.
Is MK-677 safe to take? MK-677 (ibutamoren) is NOT FDA-approved as a dietary supplement or prescription drug. It elevates fasting glucose and insulin — a meaningful risk for men over 40 with metabolic vulnerability — and is sold as a research chemical not for human use. Long-term safety in aging men has not been adequately studied.
Are collagen peptides worth taking for men? For joint recovery and connective tissue support alongside resistance training, the evidence in middle-aged and older men is reasonably strong. Collagen peptides will not replace whey for muscle protein synthesis, but they serve a different purpose. The risk profile at 10-15 g/day is minimal.
Is ipamorelin safer than other GHRPs? Ipamorelin has a more selective GH-releasing profile with less effect on cortisol and prolactin (PMID 9849822). Safer than alternatives does not mean safe or approved for human use: ipamorelin still has no approved therapeutic indication and is not a dietary supplement.
How do I know if I have low testosterone? Ask a physician for a morning serum total testosterone test on two separate days. Symptoms alone — fatigue, body composition changes, reduced libido — are not specific enough, as they overlap with sleep deficiency, metabolic syndrome, thyroid dysfunction, and depression.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion: The Bottom Line on Peptides for Men Over 40
The peptide category that works for men over 40 is narrower than the marketing suggests, and the category most aggressively marketed is the one with the least clinical support for human use.
Oral collagen peptides have a legitimate place for aging men who train: the joint recovery and connective tissue data is real, the safety record is clean, and the combination with resistance training in older cohorts produces meaningful body composition results. Treat collagen as a connective tissue supplement — not a hormonal intervention.
GHRPs (CJC-1295, ipamorelin, MK-677) raise IGF-1 in controlled settings but lack adequate long-term human data, carry metabolic safety signals, and are not approved for therapeutic use. The gap between "raises a biomarker" and "produces durable functional benefit safely" is where the grey-market peptide industry operates.
Testosterone replacement therapy is a real, evidence-based treatment for men with documented hypogonadism — and it has nothing to do with peptides.
The strongest interventions for GH output, body composition, and recovery in healthy men over 40 remain resistance training, adequate sleep, sufficient dietary protein, and where indicated, physician-supervised treatment of documented hormonal deficiencies.
Next steps:
- Understand how peptides work at a biological level before evaluating any specific compound
- Read the evidence breakdown in best peptide supplements to compare categories by clinical support
- If muscle-building is the primary goal, see peptides for muscle growth for what the evidence says on the topic specifically
- If libido or sexual health is the concern, peptides for libido covers the relevant research and regulatory context
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
