Tirzepatide is the second peptide approved by the FDA for weight management and the first to outperform semaglutide head-to-head in a large randomized trial. The honest answer to whether that difference matters for you depends on what you can tolerate, what your insurance covers, and what your physician monitors. A 6.5-percentage-point advantage in mean weight loss over 72 weeks is clinically meaningful for some patients and financially out of reach for others. This guide explains the mechanism, reviews the trial evidence, covers every safety flag in the FDA labeling, and addresses the compounded tirzepatide market — so you can have an informed conversation with your prescriber.
Summary
Tirzepatide (brands: Mounjaro for type 2 diabetes, Zepbound for weight management and obstructive sleep apnea) is a once-weekly injectable peptide that activates two distinct hormone receptors simultaneously. The clinical data are among the strongest ever generated for a weight-loss medication, and the safety profile is well-characterized but includes serious warnings you need to know before starting.
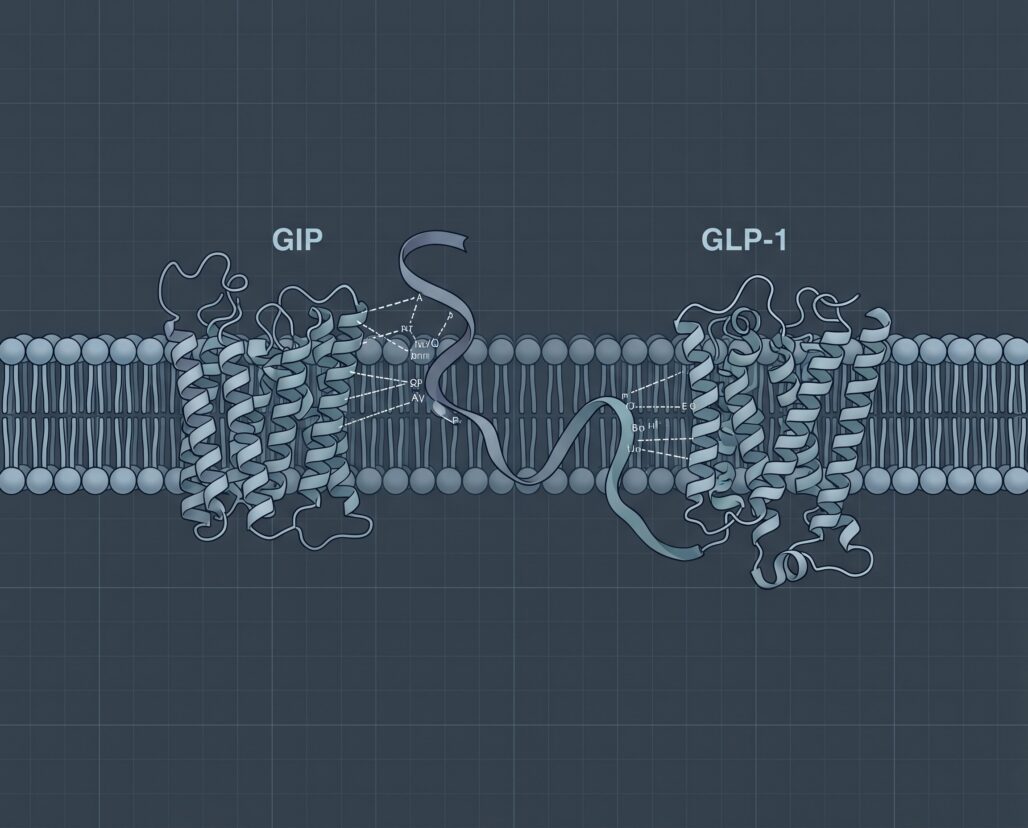
- What it is: A synthetic 39-amino-acid peptide that acts as a dual agonist at both the glucose-dependent insulinotropic polypeptide (GIP) receptor and the glucagon-like peptide-1 (GLP-1) receptor.
- What the trials showed: Mean body weight reduction of 15 to 21 percent over 72 weeks in people with obesity, depending on dose; HbA1c reductions of 2.0 to 2.3 percentage points in type 2 diabetes trials; significant reductions in sleep apnea severity.
- Head-to-head vs. semaglutide: In SURMOUNT-5 (NCT05822830), tirzepatide produced 20.2% mean weight loss versus 13.7% with semaglutide 2.4 mg over 72 weeks, a difference of approximately 6.5 percentage points (p less than 0.001).
- Key safety flags: Thyroid C-cell tumor risk (contraindicated in MEN-2 and personal/family history of medullary thyroid carcinoma), pancreatitis, hypoglycemia with insulin or sulfonylureas, reduced oral contraceptive efficacy requiring a backup method, and gastroparesis risk.
- Compounded versions: The FDA has issued specific warnings about compounded tirzepatide; these products are not FDA-approved and carry manufacturing and dosing risks not present in the branded products.
- Bottom line: Tirzepatide is a legitimate, rigorously tested prescription medicine with a meaningful efficacy advantage over the only head-to-head comparator tested to date. It is not a supplement, not available without a prescription from a licensed physician, and not safe to source outside a licensed pharmacy.
What Tirzepatide Is: Dual GIP/GLP-1 Agonism
Most people have heard of GLP-1 receptor agonists, the class that includes semaglutide and liraglutide. Tirzepatide works on that receptor too, but it adds a second one: the receptor for glucose-dependent insulinotropic polypeptide, abbreviated GIP.
Both GIP and GLP-1 are incretin hormones released by the gut after eating. They prompt the pancreas to release insulin in proportion to circulating glucose. That glucose-dependence is why these drugs carry lower hypoglycemia risk than older secretagogues: the insulin response turns down when blood glucose normalizes.
GLP-1 receptor activation reduces appetite, slows gastric emptying, and increases insulin secretion. GIP receptor activation appears to amplify those effects through a distinct pathway; preclinical data suggest it may also enhance fat metabolism in adipose tissue. The SURMOUNT-1 data support the additive effect conceptually: weight losses of 15 to 21 percent over 72 weeks exceeded what had been observed in comparably designed trials with single-receptor GLP-1 agents.
Tirzepatide is a 39-amino-acid synthetic peptide engineered with a C20 fatty diacid moiety attached through a linker, which prolongs its half-life to roughly five days and enables once-weekly dosing. For more on how synthetic peptide design enables therapeutic use, see what are peptides and FDA-approved peptides.
How Dual Agonism Differs from Semaglutide
Semaglutide is a pure GLP-1 receptor agonist. It does not activate the GIP receptor at any therapeutic dose. That distinction is pharmacologically straightforward, but its clinical significance was debated until SURMOUNT-5 provided a direct comparison.
Critics argued that SURMOUNT's superior results could reflect dose selection bias: tirzepatide was compared to lower semaglutide doses, not Wegovy at its maximum 2.4 mg dose. SURMOUNT-5 resolved that question. Randomizing 751 adults to tirzepatide 10 or 15 mg versus semaglutide 1.7 or 2.4 mg for 72 weeks, it found that tirzepatide produced mean weight loss of 20.2% versus 13.7% — a difference of approximately 6.5 percentage points (p less than 0.001). Participants on tirzepatide were significantly more likely to reach every threshold: 10%, 15%, 20%, and 25% body weight loss.
A 6.5-percentage-point population mean advantage does not guarantee any individual will lose more weight on tirzepatide. Individual response to both agents varies substantially. The SURMOUNT-5 result describes what happens at a population level with random assignment, not a personal prediction.
Some researchers propose that GIP receptor activation attenuates nausea, the most common reason patients discontinue GLP-1 therapy. Trial data do not clearly support a lower discontinuation rate for tirzepatide versus semaglutide, so this hypothesis remains preliminary.
Branded Products: Mounjaro and Zepbound
Both Mounjaro and Zepbound contain tirzepatide as the active ingredient. They are manufactured by Eli Lilly and Company and share the same molecule, the same delivery device (autoinjector pen), the same dosing intervals, and the same boxed warning. The difference is entirely in the approved indication.
| Brand | Indication | Approval year | Starting dose | Dose ramp | Max dose |
|---|---|---|---|---|---|
| Mounjaro | Type 2 diabetes (adults and pediatric patients 10+) | 2022 | 2.5 mg weekly x 4 weeks | +2.5 mg every 4 weeks minimum | 15 mg weekly (adults); 10 mg (pediatric) |
| Zepbound | Chronic weight management (obesity or overweight with comorbidity) | 2023 | 2.5 mg weekly x 4 weeks | +2.5 mg every 4 weeks minimum | 15 mg weekly |
| Zepbound | Moderate-to-severe obstructive sleep apnea (adults with obesity) | 2024 | 2.5 mg weekly x 4 weeks | +2.5 mg every 4 weeks minimum | 15 mg weekly (maintenance: 10 or 15 mg) |
The Mounjaro approval came in May 2022, making tirzepatide the first dual GIP/GLP-1 agonist approved anywhere in the world. Zepbound for weight management followed in November 2023, and the obstructive sleep apnea indication was added in December 2024 — the first drug approval specifically for OSA in adults with obesity.
Prescribers sometimes write Mounjaro for weight management as an off-label use when insurance coverage differs. This is legal; discuss with your pharmacist to confirm what is covered under your plan.
Major Trial Results: SURPASS, SURMOUNT, and SURMOUNT-OSA
SURPASS Program (Type 2 Diabetes)
The SURPASS program supported the Mounjaro NDA across multiple international trials in adults with type 2 diabetes.
SURPASS-2 (NCT03987919), published in the New England Journal of Medicine in August 2021 (PMID 34170647), compared tirzepatide 5, 10, and 15 mg to semaglutide 1 mg weekly in 1,879 adults over 40 weeks. HbA1c reductions were -2.01, -2.24, and -2.30 percentage points respectively versus -1.86 for semaglutide 1 mg. Weight loss was also greater at all tirzepatide doses, with the 15 mg dose producing approximately 5.5 kg more than semaglutide 1 mg. That comparison used the diabetes dose of semaglutide; SURMOUNT-5 later addressed the higher obesity dose directly.
SURMOUNT Program (Weight Management)
SURMOUNT-1 (NCT04184622) was the primary efficacy trial supporting the Zepbound weight management NDA. Published in the New England Journal of Medicine on July 21, 2022 (PMID 35658024), it enrolled 2,539 adults with obesity (mean BMI 38.0) but without type 2 diabetes and randomized them to tirzepatide 5, 10, or 15 mg or placebo over 72 weeks.
The results were notable. Mean weight loss at 72 weeks was:
- 5 mg tirzepatide: 15.0% versus 3.1% placebo
- 10 mg tirzepatide: 19.5% versus 3.1% placebo
- 15 mg tirzepatide: 20.9% versus 3.1% placebo
At the 10 mg and 15 mg doses, 50% and 57% of participants respectively achieved at least 20% body weight reduction. Those figures had not been seen in a phase 3 trial for any prior weight-loss medication. All comparisons with placebo were statistically significant (p less than 0.001).
SURMOUNT-OSA (Obstructive Sleep Apnea)
The SURMOUNT-OSA program (NCT05412004), published in the New England Journal of Medicine in October 2024 (PMID 38912654), enrolled 469 adults with moderate-to-severe obstructive sleep apnea and obesity across two parallel trials: one in patients not using positive airway pressure therapy and one in patients on background PAP therapy.
In the PAP-naive group, tirzepatide reduced the apnea-hypopnea index (AHI, the standard measure of sleep apnea severity) by 25.3 events per hour versus a 5.3 reduction with placebo, a treatment difference of 20.0 events per hour (p less than 0.001). In the PAP-ongoing group, tirzepatide reduced AHI by 29.3 events per hour versus 5.5 with placebo, a treatment difference of 23.8 events per hour (p less than 0.001). These reductions were accompanied by significant improvements in body weight, hypoxic burden, C-reactive protein, and systolic blood pressure.
This trial supported the December 2024 FDA approval of Zepbound for obstructive sleep apnea, making it the first drug to carry that specific indication.
SURMOUNT-5 (Head-to-Head vs. Semaglutide)
SURMOUNT-5 (NCT05822830) directly compared tirzepatide to semaglutide at its highest approved weight-loss dose. Published in the New England Journal of Medicine in July 2025 (PMID 40353578) and funded by Eli Lilly, it enrolled 751 adults with obesity randomized to tirzepatide 10 or 15 mg versus semaglutide 1.7 or 2.4 mg for 72 weeks.
Tirzepatide produced mean weight loss of 20.2% versus 13.7% for semaglutide, a difference of approximately 6.5 percentage points (p less than 0.001). Participants on tirzepatide were significantly more likely to reach the 10%, 15%, 20%, and 25% body weight reduction thresholds. The primary endpoint — mean percentage weight change — is objective; Lilly funding is worth noting for secondary endpoints.
Side Effects and the Boxed Warning
Boxed Warning: Thyroid C-Cell Tumors
The FDA requires a boxed warning on both Mounjaro and Zepbound regarding thyroid C-cell tumors. In rodent studies, tirzepatide caused dose-dependent and duration-dependent thyroid C-cell tumors at clinically relevant exposures. Whether this finding translates to humans is not yet known; the rodent data did not arise in other species studied, and GLP-1 receptors are expressed at very low levels in human thyroid tissue compared to rodent thyroid.
Because the human risk cannot be excluded, tirzepatide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). If you have a family history of thyroid cancer, you need to clarify the specific type with your physician before starting tirzepatide. Most thyroid cancers are papillary or follicular, not medullary, and the contraindication applies specifically to medullary carcinoma.
Pancreatitis
Acute pancreatitis, including fatal cases, has been reported in tirzepatide clinical programs and in post-marketing surveillance for the GLP-1 class broadly. The prescribing information instructs clinicians to discontinue tirzepatide immediately if pancreatitis is suspected and not to restart it if pancreatitis is confirmed. Symptoms to watch for include persistent abdominal pain, especially if it radiates to the back, nausea, and vomiting. This is not a reason to avoid tirzepatide if your physician believes you are an appropriate candidate, but it is a reason to seek evaluation promptly if those symptoms develop.
Hypoglycemia with Insulin or Sulfonylureas
Tirzepatide on its own carries a low risk of clinically significant hypoglycemia because its insulin-stimulating effect is glucose-dependent: it turns down when blood glucose normalizes. The risk rises substantially when tirzepatide is combined with insulin or a sulfonylurea (such as glipizide or glimepiride), drugs that do not share that glucose-dependence. The prescribing information recommends reducing the dose of the insulin or sulfonylurea when starting tirzepatide to lower this risk.
Oral Contraceptive Absorption
The Mounjaro and Zepbound prescribing information contains a specific warning about oral hormonal contraceptives. Tirzepatide delays gastric emptying, which can reduce the rate at which oral medications are absorbed, including combined oral contraceptive pills. The FDA label advises that females using oral hormonal contraceptives should switch to a non-oral contraceptive method or add a barrier method for four weeks after initiating tirzepatide and for four weeks after each dose escalation. This warning applies during the dose ramp-up period specifically because the degree of gastric emptying delay is most pronounced at lower doses before tolerance develops. Discuss a concrete contraception plan with your prescriber before starting.
Delayed Gastric Emptying and Gastroparesis
Tirzepatide slows gastric emptying as part of its mechanism of action. In patients who already have gastroparesis (severely delayed stomach emptying, often seen in long-standing diabetes), this effect can worsen symptoms substantially. The prescribing information states that tirzepatide is not recommended in patients with severe gastroparesis. Case reports in the published literature following Zepbound's approval have documented new or worsened gastroparesis symptoms requiring hospitalization, so this is an active monitoring concern rather than a theoretical one.
Pregnancy
Animal reproductive studies have shown potential fetal harm at tirzepatide exposures comparable to clinical doses. Women who are pregnant or planning to become pregnant should not use tirzepatide. Because tirzepatide has a half-life of approximately five days, meaningful washout before conception requires stopping the drug well in advance — generally at least one to two months is discussed in clinical guidance, though your physician should advise on specific timing based on your situation. For the same reason, do not start tirzepatide if there is any possibility you could be pregnant, and discuss family planning with your prescriber before beginning treatment.
Common Adverse Effects
The most frequently reported adverse events across the SURMOUNT and SURPASS trials were gastrointestinal: nausea, diarrhea, vomiting, and constipation. These effects are most common during dose escalation and tend to improve after reaching a stable maintenance dose. In SURMOUNT-1, approximately 4 to 5 percent of participants discontinued tirzepatide due to gastrointestinal adverse events. That is a meaningful number: not everyone tolerates the escalation.
Compounded Tirzepatide: What the FDA Has Said
When tirzepatide was on the FDA drug shortage list, compounding pharmacies could legally prepare copies under specific conditions. The FDA removed tirzepatide from the shortage list, ending the legal basis for most compounding. The agency has since warned that compounded versions are not FDA-approved: they have not been verified for potency, sterility, or dose accuracy.
Some compounding pharmacies operate carefully under state board oversight. But the record for compounded injectables includes documented cases of incorrect concentrations, contamination, and label errors — a concerning profile for a drug with a specific dose escalation ladder and real safety requirements. If you are currently using compounded tirzepatide, the actionable takeaway is not to stop abruptly without physician guidance, but to understand that it is an unverified product and to ask your prescriber about patient assistance programs for the branded versions.
Practical Considerations for Starting Tirzepatide
If you and your physician decide tirzepatide is appropriate, a few practical points can make a meaningful difference:
Dose escalation pace matters. The approved schedule is 2.5 mg weekly for four weeks, then up by 2.5 mg every four weeks minimum until you reach your maintenance dose. Moving faster than that schedule increases gastrointestinal side effects without meaningfully accelerating weight loss.
Dietary pattern interacts with tolerability. High-fat, high-calorie meals worsen nausea and vomiting on tirzepatide. Patients who eat smaller meals with lower fat content during the escalation phase report substantially better tolerability.
Muscle mass monitoring is clinically important. A significant portion of weight lost on tirzepatide includes lean mass. This is reason to discuss resistance exercise and adequate protein intake with your physician throughout treatment. For more on this issue, see peptides for weight loss.
Insurance prior authorization is almost universal. Both Mounjaro and Zepbound require prior authorization from nearly all commercial payers in the United States. Criteria commonly include BMI thresholds, documented comorbidities, and prior intervention history. Expect the process to take days to weeks.

Frequently Asked Questions
Can I take tirzepatide if I have type 2 diabetes and want to lose weight? Yes. Mounjaro is approved for type 2 diabetes and also produces significant weight loss. Some physicians and insurers prefer prescribing Mounjaro for patients with diabetes and Zepbound for patients without. The clinical effect is the same drug; the coverage path differs.
How is tirzepatide different from Ozempic? Ozempic contains semaglutide, a pure GLP-1 receptor agonist. Tirzepatide adds GIP receptor agonism on top of GLP-1 agonism. In SURMOUNT-5, tirzepatide at doses up to 15 mg outperformed semaglutide at doses up to 2.4 mg (the Wegovy weight-loss dose) by approximately 6.5 percentage points of mean body weight loss over 72 weeks.
Is tirzepatide a peptide? Yes. It is a synthetic 39-amino-acid peptide, placing it in the same chemical class as insulin and semaglutide. For a broader explanation, see what are peptides.
What happens if I stop taking tirzepatide? Clinical trials consistently show that stopping tirzepatide leads to weight regain toward baseline over subsequent months. The same pattern is seen with all GLP-1-class agents. Tirzepatide manages weight while it is being taken; it is not a one-time course.
How long does it take to see results? Most patients on higher maintenance doses see meaningful weight loss by weeks 12 to 16. Maximum efficacy in SURMOUNT trials was measured at 72 weeks. The dose escalation period is a prerequisite, not a delay.
Is tirzepatide approved for children? Mounjaro is approved for pediatric patients aged 10 and older with type 2 diabetes, maximum dose 10 mg weekly. Zepbound does not currently carry a pediatric indication.
If you are managing a protocol like this, StackMyMed (our companion app) keeps your doses, timing, and interaction checks in one place. It does not replace medical advice — bring the log to your clinician.
Conclusion
Tirzepatide represents a genuine step forward in pharmacological weight management and type 2 diabetes treatment. The dual GIP/GLP-1 mechanism produced superior weight loss in a well-conducted head-to-head trial against the leading alternative at its maximum dose. The SURMOUNT program generated some of the strongest phase 3 efficacy data recorded for a weight-loss medication, and the SURMOUNT-OSA approval opened a clinical use case no prior drug could claim.
Tirzepatide has real safety requirements: a boxed warning that demands screening for thyroid cancer history, a pancreatitis risk requiring prompt recognition, a drug interaction with oral contraceptives requiring a concrete backup plan, and a dose-escalation period that causes roughly one in twenty patients to discontinue. These are manageable with appropriate prescriber monitoring.
Sourcing tirzepatide outside a licensed U.S. pharmacy with a valid prescription is not a shortcut; it is a path to an unverified product. The conversation about whether tirzepatide is right for you belongs with a physician who knows your full medical history.
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
