Both drugs are weekly GLP-1 injections, both treat type 2 diabetes, and both land in the same pharmacy aisle. So when a patient asks "what is actually different between Ozempic and Trulicity?", the honest answer is: more than the brand names suggest, and the trial data makes those differences measurable. That said, the comparison only matters inside a conversation with your prescribing physician.
The honest answer: semaglutide (Ozempic) produced significantly greater HbA1c reduction and weight loss than dulaglutide (Trulicity) in the most rigorous head-to-head trial available, but both drugs reduced cardiovascular events in large outcomes studies, and Trulicity's cardiovascular label covers a broader patient population. Individual tolerance, device preference, insurance placement, and physician judgment are the decisive variables at the prescription level.
Summary
- Ozempic is semaglutide, a GLP-1 receptor agonist, FDA-approved for type 2 diabetes in adults: glycemic control and cardiovascular risk reduction in those with established CVD. It is not FDA-approved for weight loss as Ozempic — that is Wegovy, a separate labeled product.
- Trulicity is dulaglutide, also a GLP-1 receptor agonist, FDA-approved for type 2 diabetes in adults and pediatric patients aged 10 and older, with a cardiovascular indication that includes patients with multiple CV risk factors, not only those with established disease. Trulicity has no weight-loss-labeled sister brand.
- Both carry a boxed warning for thyroid C-cell tumors, share pancreatitis warnings, and are contraindicated in personal or family history of medullary thyroid carcinoma (MTC) or MEN 2.
- In SUSTAIN 7 (NCT02648204), a 40-week head-to-head randomized trial, semaglutide outperformed dulaglutide on HbA1c reduction and body weight at every dose pair tested (Pratley et al., Lancet Diabetes Endocrinol, 2018, PMID 29397376).
- Both drugs reduced MACE in large cardiovascular outcomes trials (SUSTAIN 6 and REWIND) with different patient populations — direct numerical cross-comparison is not appropriate.
- Neither drug is available without a prescription. Both require ongoing physician supervision and monitoring.
Both Products at a Glance
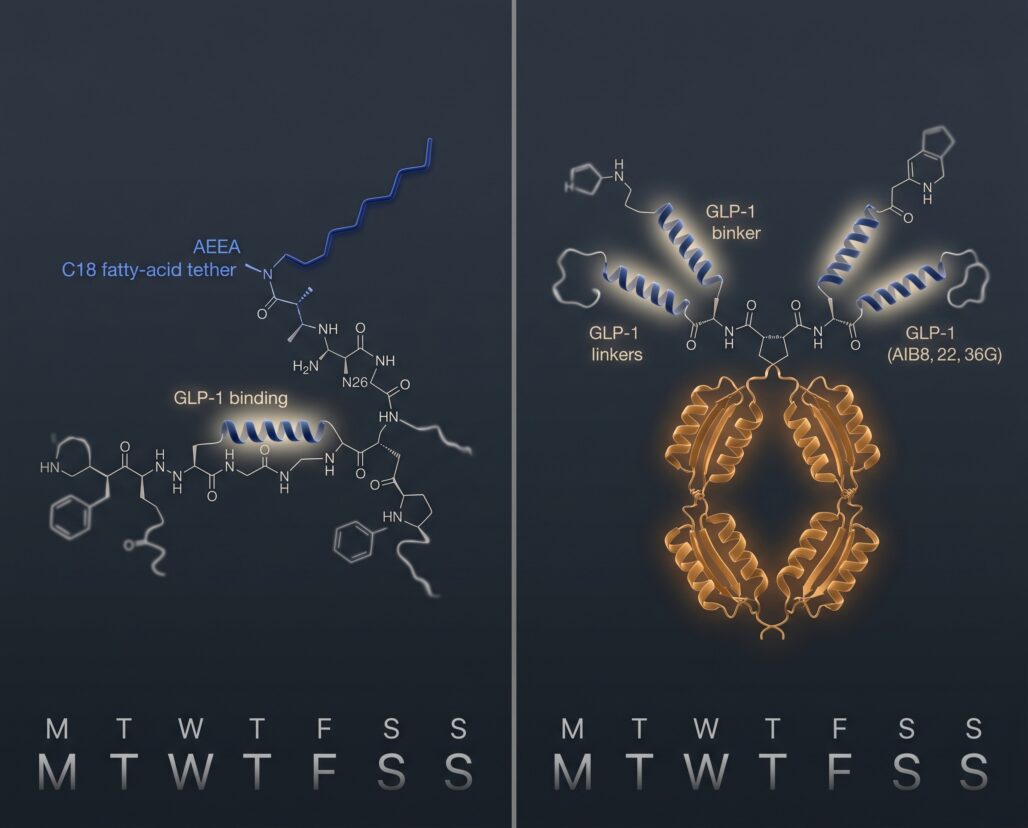
Ozempic (semaglutide) received FDA approval in December 2017 and is manufactured by Novo Nordisk. Semaglutide is a synthetic GLP-1 analogue with a C18 fatty-acid side chain that enables albumin binding, extending the half-life to roughly seven days and making once-weekly dosing possible. The prescribing information specifies starting at 0.25 mg weekly for four weeks as a tolerability step, then advancing to 0.5 mg, with 1 mg and 2 mg available for additional glycemic control.
Trulicity (dulaglutide) received FDA approval in September 2014 and is manufactured by Eli Lilly. Dulaglutide fuses the GLP-1 analogue sequence to a modified human IgG4 Fc region, creating a larger protein that resists enzymatic degradation with a half-life compatible with weekly dosing. Starting dose is 0.75 mg weekly, increasing to 1.5 mg after four weeks; doses up to 4.5 mg have since been approved.
Both molecules work through the GLP-1 receptor on pancreatic beta cells and hypothalamic neurons, stimulating glucose-dependent insulin release, suppressing glucagon, and slowing gastric emptying. The differences in efficacy between the two drugs reflect distinctions in binding affinity and pharmacokinetics, not a fundamentally different mechanism.
Head-to-Head Efficacy: SUSTAIN 7
SUSTAIN 7 (NCT02648204) is the pivotal direct comparison, published in The Lancet Diabetes and Endocrinology in April 2018 by Pratley and colleagues (PMID 29397376). The trial enrolled 1,201 adults with type 2 diabetes inadequately controlled on metformin, randomized to semaglutide 0.5 mg or 1.0 mg weekly versus dulaglutide 0.75 mg or 1.5 mg weekly. Primary endpoint: HbA1c change at week 40. Key secondary: body weight.
HbA1c at week 40:
- Semaglutide 0.5 mg: -1.5 pp vs. dulaglutide 0.75 mg: -1.1 pp (difference: -0.40 pp; p less than 0.0001)
- Semaglutide 1.0 mg: -1.8 pp vs. dulaglutide 1.5 mg: -1.4 pp (difference: -0.41 pp; p less than 0.0001)
Weight loss at week 40:
- Semaglutide 0.5 mg: -4.6 kg vs. dulaglutide 0.75 mg: -2.3 kg (difference: -2.26 kg; p less than 0.0001)
- Semaglutide 1.0 mg: -6.5 kg vs. dulaglutide 1.5 mg: -3.0 kg (difference: -3.55 kg; p less than 0.0001)
At the higher dose pair, semaglutide produced roughly twice the weight reduction. One caveat worth stating: SUSTAIN 7 was not a weight-loss trial. Ozempic is not FDA-approved for weight management — Wegovy is. The weight figures are secondary outcomes from a glycemic control study in T2D patients on metformin, not people seeking obesity treatment. GI adverse event rates were broadly similar across arms (43-44% for semaglutide vs. 33-48% for dulaglutide), with GI events driving most discontinuations in both groups.
Cardiovascular Outcomes: SUSTAIN 6 vs. REWIND
Neither Ozempic nor Trulicity was evaluated against each other in a cardiovascular outcomes trial. Each drug has its own dedicated CVOT, and the populations enrolled in those trials differed enough that direct numerical comparison is not appropriate. What the trials do confirm is that both drugs can be used in patients with cardiovascular risk — a clinically significant question for type 2 diabetes management.
SUSTAIN 6 (NCT01720446) enrolled 3,297 adults with type 2 diabetes and high cardiovascular risk. Of those, 83% had established cardiovascular disease, chronic kidney disease, or both — a high-risk population. Over 104 weeks, semaglutide 0.5 mg or 1.0 mg reduced MACE (cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) versus placebo: 6.6% vs. 8.9%, hazard ratio 0.74 (95% CI 0.58-0.95; p less than 0.001 for noninferiority). The reduction was driven primarily by nonfatal stroke. However, semaglutide was also associated with a higher rate of retinopathy complications (HR 1.76; p=0.02), a finding that is included in the prescribing information (PMID 27633186).
REWIND (NCT01394952) enrolled 9,901 adults with type 2 diabetes aged 50 or older. Critically, the REWIND population included patients with established cardiovascular disease and those with only cardiovascular risk factors — a broader and generally lower-risk group than SUSTAIN 6. Median follow-up was 5.4 years, the longest of any GLP-1 CVOT at the time. Dulaglutide 1.5 mg reduced the primary composite endpoint versus placebo: 12.0% vs. 13.4%, hazard ratio 0.88 (95% CI 0.79-0.99; p=0.026) (PMID 31189511). The REWIND result translated directly into Trulicity's cardiovascular indication, which covers patients with multiple risk factors rather than only those with established disease — a broader labeled population than Ozempic's cardiovascular indication.
Comparing the hazard ratios from SUSTAIN 6 and REWIND as if they measure the same thing is a statistical error: different enrollment criteria, follow-up durations, and baseline risk levels make cross-trial HR comparisons unreliable. What the trials share is the conclusion that both drugs carry a cardiovascular indication backed by randomized outcomes data.
Side Effects Compared
Both drugs share a GLP-1-mediated side-effect profile dominated by gastrointestinal events: nausea, diarrhea, vomiting, constipation, and abdominal pain. These are most common during dose escalation and typically diminish over time, though a meaningful minority stops treatment because of them. In SUSTAIN 7, GI disorders affected roughly 43-44% of semaglutide patients and 33-48% of dulaglutide patients across dose arms.
Two warnings apply to both drugs and require explicit understanding before starting either:
Thyroid C-cell tumors (boxed warning): Rodent studies showed dose-dependent thyroid C-cell tumors with both semaglutide and dulaglutide. Human relevance is unknown. Both drugs are contraindicated in personal or family history of medullary thyroid carcinoma or MEN 2. Report any neck mass, dysphagia, or hoarseness to a physician promptly.
Pancreatitis: Both labels warn that acute pancreatitis — including fatal and nonfatal hemorrhagic or necrotizing cases — has been observed with GLP-1 receptor agonists. Discontinue if pancreatitis is suspected; do not restart if confirmed.
Additional shared warnings: retinopathy complications in patients with pre-existing retinopathy (most clearly documented for semaglutide in SUSTAIN 6), hypoglycemia when combined with insulin or sulfonylureas, and acute kidney injury from GI-related dehydration. Both drugs should be discontinued before a planned pregnancy: Ozempic's prescribing information recommends stopping at least two months before conception due to semaglutide's long washout period; Trulicity's label recommends discontinuation as well given animal data showing fetal risk.
Devices and Dosing
The delivery device is not a trivial detail for patients who will be injecting a medication every week, potentially for years. Ozempic and Trulicity use meaningfully different delivery systems.
Ozempic comes in a prefilled, disposable, single-patient-use pen injector. Each pen contains multiple doses; patients dial to the prescribed dose and attach a needle before each injection. It is designed for use in the abdomen, thigh, or upper arm.
Trulicity uses a single-dose auto-injector with a concealed, pre-attached needle. Patients press the device against the skin and click the button — no exposed needle handling. Each device is used once and discarded. This design was built specifically to reduce injection anxiety and is frequently cited in patient preference surveys as a reason for choosing Trulicity.
Neither system is objectively better. Patients comfortable with multi-dose pen injectors (for example, those with prior insulin experience) tend to find Ozempic familiar. Patients new to injectable medications, or those with needle anxiety, often prefer Trulicity's auto-injector. Adherence to a weekly schedule is the variable most within a patient's control, so device preference is a legitimate consideration to raise with your prescriber. Both drugs are refrigerated before first use; at room temperature, Ozempic stays viable for up to 56 days, Trulicity for 14 days.
Cost and Insurance Reality
Neither Ozempic nor Trulicity has an FDA-approved generic as of 2026. Monthly list prices for both sit in the $900-$1,000 range, though very few patients pay list price. What patients actually pay depends on insurance formulary tier, prior authorization status, and manufacturer savings programs. Novo Nordisk offers an Ozempic savings card for eligible commercially insured patients; Eli Lilly offers an equivalent program for Trulicity. Medicare and Medicaid beneficiaries are typically excluded from these savings programs. Prior authorizations often require documentation of prior diabetes therapy or minimum HbA1c thresholds and vary substantially by payer.
The FDA has issued explicit cautions about compounded semaglutide products sold outside Ozempic and Wegovy's approved labeling: they are not FDA-approved, have not been evaluated for safety or efficacy, and have been linked to adverse events including hospitalizations. Compounded dulaglutide products raise the same concerns. Neither should be used without physician supervision and clear awareness of the risks.
Side-by-Side Comparison Table
| Property | Ozempic (semaglutide) | Trulicity (dulaglutide) |
|---|---|---|
| Active ingredient | Semaglutide | Dulaglutide |
| Manufacturer | Novo Nordisk | Eli Lilly |
| FDA approval (T2D) | December 2017 | September 2014 |
| Molecule type | GLP-1 analogue (fatty-acid tethered) | GLP-1 / IgG4 Fc fusion protein |
| FDA-approved for weight loss | No (Wegovy is the weight-loss brand) | No (no weight-loss-labeled sister brand) |
| Starting dose | 0.25 mg once weekly | 0.75 mg once weekly |
| Maximum approved dose | 2 mg once weekly | 4.5 mg once weekly |
| Delivery device | Multi-dose prefilled pen injector | Single-dose auto-injector (concealed needle) |
| HbA1c reduction (SUSTAIN 7) | 1.5-1.8 pp | 1.1-1.4 pp |
| Weight loss (SUSTAIN 7) | 4.6-6.5 kg | 2.3-3.0 kg |
| CV outcomes trial | SUSTAIN 6 (high-risk T2D, 83% established CVD) | REWIND (T2D with CVD or risk factors) |
| MACE hazard ratio | 0.74 (vs. placebo) | 0.88 (vs. placebo) |
| Thyroid C-cell tumor warning | Yes (boxed warning) | Yes (boxed warning) |
| Pancreatitis warning | Yes | Yes |
| Retinopathy warning | Yes (from SUSTAIN 6 data) | Less prominent in label |
| Pediatric approval | No | Yes (10 years and older) |
| Approximate list price/month | ~$900-$1,000 | ~$900-$1,000 |

Frequently Asked Questions
Can I switch from Trulicity to Ozempic or vice versa?
Switching is common in clinical practice but requires physician guidance on timing, dose, and monitoring. Do not self-adjust based on online comparisons.
Is semaglutide always the stronger choice given SUSTAIN 7?
Not necessarily. SUSTAIN 7 tested specific dose pairs in T2D patients on metformin over 40 weeks. A patient who cannot tolerate semaglutide's GI effects, has contraindications, or whose insurer only covers dulaglutide will not benefit from those trial averages. Population means do not predict individual responses.
What about Trulicity's broader cardiovascular indication?
Trulicity's label covers patients with established CVD or multiple cardiovascular risk factors; Ozempic's cardiovascular indication requires established CVD. This distinction matters for some prescribers and payers at the formulary level.
Are compounded versions safe?
The FDA has issued explicit cautions: compounded semaglutide is not FDA-approved and has been linked to hospitalizations. The same concerns apply to compounded dulaglutide. Discuss any compounded GLP-1 product with your physician before use.
Do both drugs require dietary and lifestyle changes?
Yes. Both labels describe these drugs as adjuncts to diet and exercise, not replacements. Trial benefits were achieved alongside dietary management.
Conclusion
Ozempic and Trulicity are genuine peers in the weekly GLP-1 class, with meaningful differences at the prescription level. SUSTAIN 7 (PMID 29397376) provides the clearest signal: semaglutide produced approximately 0.4 percentage points greater HbA1c reduction and 2.3 to 3.5 kg greater weight loss versus dulaglutide over 40 weeks. Both drugs demonstrated cardiovascular benefit — SUSTAIN 6 (PMID 27633186) for semaglutide and REWIND (PMID 31189511) for dulaglutide — though those trials enrolled different populations and their hazard ratios cannot be directly compared.
For the full semaglutide clinical picture, see the semaglutide complete guide and the dulaglutide guide. If your prescriber is weighing a dual-agonist, the Ozempic vs. Mounjaro comparison covers tirzepatide using SURPASS-2 data.
Actionable takeaways:
- Ask your physician which drug fits your HbA1c history, cardiovascular risk profile, and GI tolerance — not which scored higher in a trial your population wasn't enrolled in.
- Check your insurance formulary tier for both drugs before assuming either is accessible; prior authorization requirements change frequently.
- If device design matters (auto-injector vs. dial pen), say so — adherence to a weekly schedule is the variable most within your control, and device preference is a legitimate clinical consideration.
- Do not use compounded GLP-1 products without physician supervision and explicit awareness of the FDA's safety guidance.
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Ozempic and Trulicity are prescription medications approved for specific indications in adults with type 2 diabetes. They carry significant warnings, including a boxed warning regarding thyroid C-cell tumors, and are contraindicated in patients with certain personal or family medical histories. Only a licensed healthcare provider with full knowledge of your medical history can determine whether either medication is appropriate for you. Do not start, stop, or modify any prescription medication based on information read online.
