Before you decide
This article is general information, not medical advice. Your calcium needs depend on your diet, age, bone health, and other medicines, so treat the numbers here as a starting point for a conversation with your doctor or pharmacist.
The people most affected by this interaction are long-term PPI users, especially adults over 65 and anyone with osteoporosis or a past fracture. If you take omeprazole, esomeprazole, lansoprazole, pantoprazole, or rabeprazole most days, the form of calcium you buy genuinely matters.
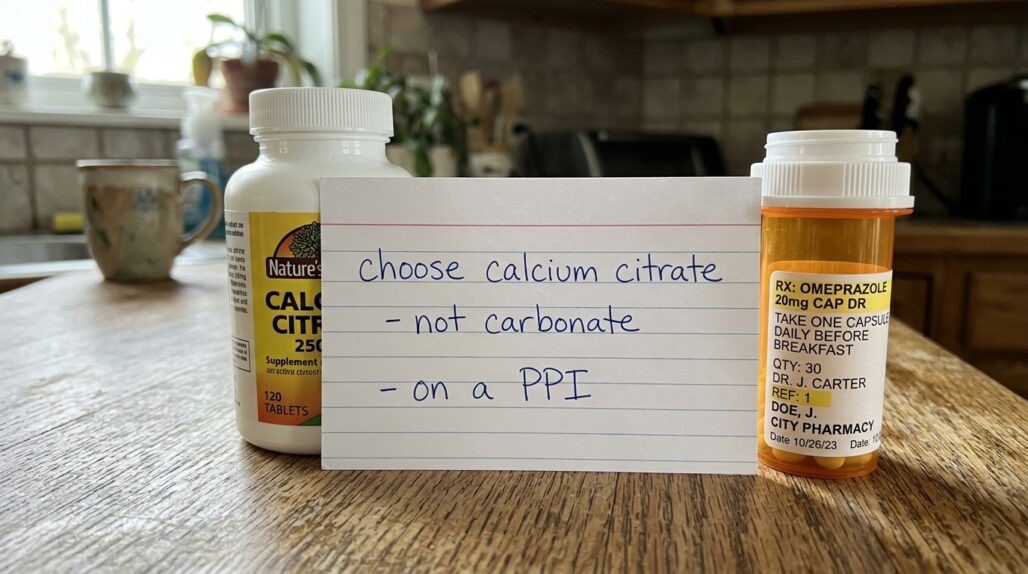
The good news: this is one of the easier interactions to manage. You do not stop the drug or skip the calcium. You switch the form and fix the timing.
How a PPI changes the way calcium absorbs
Calcium carbonate is the cheapest and most common form, and it is the antacid in Tums. To be absorbed, it first has to dissolve, and dissolving carbonate requires acid. Your stomach normally supplies that acid.
A proton pump inhibitor shuts down the pumps that make stomach acid. That is the whole point of the drug for reflux and ulcers. The side effect is that acid-dependent calcium loses its solvent.
In 1985, R.R. Recker measured this directly. In his study of calcium absorption and achlorhydria (no stomach acid), fasting patients absorbed only about 4 percent of a calcium carbonate dose, compared with roughly 45 percent from calcium citrate. People with normal acid absorbed both forms well.
Two decades later, O'Connell and colleagues confirmed the same pattern with a real PPI. Their work, a randomized crossover trial in the American Journal of Medicine, found that omeprazole 20 mg daily for a week significantly reduced absorption of calcium carbonate taken on an empty stomach in older women. Citrate was not acid-dependent and held up.
So the mechanism is settled enough to act on: no acid, no dissolved carbonate, less calcium in.

Why calcium citrate is the better pick
Calcium citrate comes pre-paired with citric acid, so it does not need your stomach to supply acid for it to dissolve. Its absorption is largely independent of gastric pH.
A clinical review on chronic PPI therapy and calcium metabolism puts it plainly: soluble calcium salts such as citrate, along with the calcium in milk and cheese, have high bioavailability regardless of gastric pH. That review is why most pharmacists steer PPI users toward citrate.
There are real trade-offs, and they are minor. Citrate has less elemental calcium per pill than carbonate (about 21 percent versus 40 percent by weight), so you may swallow a slightly larger or more frequent tablet. Many people find it gentler on the gut and less likely to cause gas or constipation.
A practical point worth knowing: even carbonate absorbs much better with a meal, because food triggers some acid release. So if cost or pill size pushes you toward carbonate, always take it with food rather than fasting.
| Feature | Calcium carbonate | Calcium citrate |
|---|---|---|
| Needs stomach acid | Yes | No |
| Good choice on a PPI | Only with food, and even then second-best | Yes, preferred |
| Elemental calcium by weight | About 40 percent | About 21 percent |
| Best taken | With a meal | With or without food |
| Gut tolerance | More gas and constipation reported | Often gentler |
The fracture worry behind all of this
The reason this question gets asked at all is bone fear. Long-term PPI use has been linked in observational studies to a higher risk of fractures, and regulators took it seriously.
In 2010 the FDA issued a drug safety communication on PPIs and fracture risk. The agency required labeling noting that people taking multiple daily doses for a year or longer may face an increased risk of fractures of the hip, wrist, and spine.
Two honest caveats. First, this is mostly observational data, which shows association rather than proof of cause. People who need years of acid suppression may differ from those who do not. Second, the size of any added risk appears modest for most users.
What follows from it is sensible, not alarming. The FDA advises using a PPI at the lowest effective dose for the shortest needed time, and keeping calcium and vitamin D adequate makes sense while you are on one. Reduced calcium absorption is one plausible piece of the fracture link, which loops right back to choosing a form your body can actually use.

What to take, and how much
Calcium works best as a team with vitamin D, which your gut needs to absorb calcium efficiently in the first place. Most calcium-for-bone products bundle the two, and that pairing is reasonable for PPI users.
Dose size matters more than people expect. According to the NIH Office of Dietary Supplements, the body absorbs calcium best in amounts of 500 mg or less at a time. If you need 1,000 mg from supplements, split it into two smaller doses across the day rather than one large pill.


As an Amazon Associate, UsefulVitamins.com earns from qualifying purchases at no extra cost to you.
UsefulVitamins may earn a commission if you buy through links on this page. It does not change what we recommend or the evidence behind it.
Aim for a sensible total, not the maximum. The recommended daily calcium intake is about 1,000 mg for most adults, rising to 1,200 mg for women over 50 and everyone over 70. That total includes the calcium in your food, so if you eat dairy or fortified foods you may need far less from pills than you think.
There is an upper boundary too. The tolerable upper intake level is 2,500 mg per day for adults up to 50 and 2,000 mg per day after that. More is not better here.
If your bone protection plan is the priority, our guides to supplements for bone health and osteoporosis prevention cover the wider picture, and the complete guide to vitamin D explains the partner nutrient.
Do not just pour on more calcium
It is tempting to fix a poor-absorbing form by simply taking more. Resist that.
Several randomized-trial meta-analyses have raised a flag about high-dose calcium supplements and the heart. A widely cited BMJ meta-analysis by Bolland and colleagues reported that calcium supplements without vitamin D were associated with a higher risk of myocardial infarction, on the order of a 27 to 31 percent relative increase in some pooled analyses.
The evidence is debated, and adding vitamin D did not clearly remove the signal in those analyses. Calcium from food has not carried the same concern.
The takeaway is balance. Cover the gap between your diet and your daily target, use a form that absorbs (citrate on a PPI), and do not stack pills past what you need. If you are unsure how much you actually get from food, a registered dietitian or pharmacist can run the numbers with you.
You can keep your full list of medicines and supplements in one place with a tool like StackMyMed, which makes it easier to flag a PPI-plus-calcium combination and bring it up at your next appointment. It helps you organize and ask better questions; it does not replace a clinician's judgment.
For a broader view of how acid-suppressing drugs affect nutrients, see our ultimate guide to drug-supplement interactions or run your own regimen through the drug-supplement interaction checker. Calcium is not the only nutrient a PPI touches; magnesium is another, covered in omeprazole and magnesium depletion.

When to get a clinician involved
Most people can switch to citrate on their own. A few situations call for a professional eye.
Loop in your doctor or pharmacist if any of these apply to you.
- You have been on a PPI for more than a year, or take more than one acid-suppressing drug.
- You have osteoporosis, low bone density, or a prior fragility fracture.
- You take other medicines that calcium can bind, such as levothyroxine, certain antibiotics, or iron (these need to be spaced apart).
- You have kidney disease or a history of kidney stones, where calcium dosing needs care.
- You are considering more than 500-600 mg per day of supplemental calcium.
Ask two questions at that visit: is the PPI still needed at this dose, and does my calcium and vitamin D plan fit my bones and my heart. Both are reasonable to revisit periodically.
FAQ
Can I take calcium carbonate at all while on omeprazole? Yes, but take it with a meal, since food prompts some acid that helps it dissolve. On a fasting stomach its absorption can fall sharply, so calcium citrate is the safer default for PPI users.
How far apart should I take calcium and my omeprazole? Spacing is less of an issue for citrate, because it does not rely on stomach acid. The bigger habit is keeping each calcium dose at 500-600 mg or less and pairing it with vitamin D.
Does calcium citrate really absorb better, or is that marketing? The difference is real on a PPI. Research suggests citrate absorbs independent of gastric pH, while carbonate absorption drops without acid. For someone with normal stomach acid and a meal, the two are much closer.
Will switching to citrate undo the PPI fracture risk? No one can promise that. Adequate, absorbable calcium plus vitamin D is a sensible part of bone protection, but the fracture link is multifactorial. Using the lowest effective PPI dose for the shortest time, with your doctor, also matters.
How much calcium should I get in total each day? About 1,000 mg for most adults, and 1,200 mg for women over 50 and everyone over 70, counting food. The upper limit is 2,000 to 2,500 mg per day depending on age, so more is not better.
Should I worry about calcium supplements and my heart? Some trial analyses have linked high-dose supplements to a modest rise in heart attack risk, though the evidence is debated and food calcium is not implicated. The practical answer is to supplement only the gap your diet leaves, not a megadose.
Conclusion: pick citrate, keep doses small, talk to your pharmacist
The interaction is simple once you see the mechanism. Omeprazole removes the stomach acid that calcium carbonate needs to dissolve, so on a PPI you want calcium citrate, which absorbs regardless of acid.
Keep each dose at 500-600 mg or less, pair calcium with vitamin D, hit your daily target without overshooting, and do not lean on the supplement to cancel out the fracture worry on its own. Bring your full list to a pharmacist, especially if you have been on the PPI long term or have bone concerns.
This article is for general education and is not a substitute for personalized medical advice. Always discuss changes to your medicines or supplements with a qualified healthcare professional.
Reviewed by the UsefulVitamins Editorial Team.
