If you spend any time in wellness corners of the internet, you have probably seen BPC-157 described as the peptide that "heals your gut from the inside." Proponents credit it with fixing everything from leaky gut to Crohn's disease. The mechanism sounds plausible — but the actual human evidence is far thinner than the marketing suggests. This article breaks down what the research genuinely shows, separates real biology from hype, and points to interventions with actual human trial data.
Summary / Quick Answer: Do Peptides Actually Fix Gut Problems?
The honest answer is: it depends on which peptide and what you mean by "gut problems." BPC-157 has extensive animal data showing anti-inflammatory and healing effects in rat gut models, but as of 2026 there are no published human RCTs confirming those effects in conditions like IBD or leaky gut. KPV, an alpha-MSH fragment, has promising cell and mouse data but zero human trials. Meanwhile, interventions like L-glutamine (in specific populations) and certain probiotic strains have multiple human RCTs supporting real, measurable improvements in gut barrier function.
Best for: People with post-infectious IBS-D or specific barrier disruption who want human-tested options.
Not ideal for: Anyone expecting BPC-157 or KPV to replicate their animal-study results in a human body — that translation has not been demonstrated.
What to look for: Human RCT data measuring actual permeability markers (lactulose/mannitol ratio, zonulin) rather than symptom scores alone.
Decision shortcut: If you are managing diagnosed IBD, IBS, or any gut condition, consult a gastroenterologist before trying any peptide or aggressive supplement protocol. Do not replace prescribed treatment with research chemicals.
"Leaky Gut" and the Marketing Pipeline
The phrase "leaky gut" gets used in two very different ways, and confusing them is how supplement marketing gains traction.
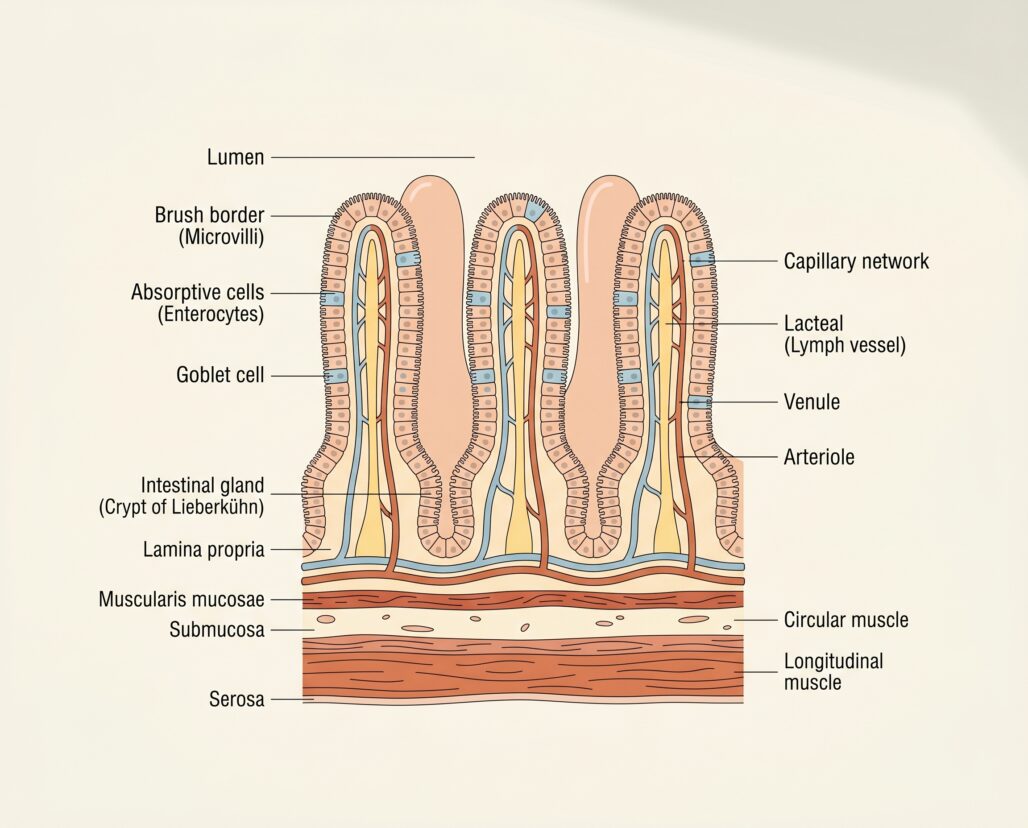
Increased intestinal permeability is a real, measurable physiological state. Your intestinal wall is not a solid wall — it is a single layer of epithelial cells linked together by protein structures called tight junctions. When those junctions loosen under stress (from NSAID use, infection, severe exercise, or inflammatory disease), larger molecules — bacterial fragments, undigested proteins, endotoxins — pass through more easily than they should. Researchers can measure this using probe molecules like lactulose and mannitol: you drink them, and the ratio recovered in your urine over the next several hours reflects how porous the small and large intestine is. A 2019 Frontiers review summarized multiple validated measurement techniques, including serum zonulin and intestinal fatty-acid binding protein as blood biomarkers. Elevated permeability is documented in IBD, celiac disease, IBS, and even in healthy endurance athletes after prolonged heat exposure.
"Leaky gut syndrome" is something different. It is a marketing label applied to a sprawling list of vague complaints — brain fog, fatigue, skin issues, mood changes — and attributed to gut permeability as the root cause. As Fasano's widely cited 2012 review (PMC6790068) makes clear, there is no gold-standard diagnostic test, no agreed clinical threshold, and "it is still unproven that restoring barrier function can ameliorate clinical manifestations" even when permeability is elevated. The phenomenon of increased permeability is legitimate. The syndrome wrapped around it is not an accepted medical diagnosis.
This distinction matters because the peptide marketing pipeline runs directly through it. A peptide shows reduced gut inflammation in mice. A supplement company frames that as "heals leaky gut." A TikTok creator adds a testimonial. None of that is a human trial showing this compound reduces measurable permeability in people with a defined gut condition.
The real question is not whether a peptide can reduce inflammation in a rodent colon. It is whether it does so in humans, at a safe and achievable dose.
BPC-157: The Animal Data vs. the Human Reality
BPC-157 (body protection compound 157) is a synthetic 15-amino-acid peptide derived from a protein found in gastric juice. The preclinical data on it is genuinely striking. A 2024 review in PMC (PMC11053547) summarizes decades of rat studies showing accelerated healing of gastric lesions, reduced NSAID-induced intestinal damage, improved anastomosis healing after bowel surgery, and normalization of gut motility. These are not trivial findings in rodents. The mechanistic pathways — involving nitric oxide synthase, vascular endothelial growth factor, and prostaglandin modulation — are biologically coherent.
The problem is translation. Animal models tell us a peptide CAN do something, not that it WILL in humans.
On the human side, the picture is sparse. The same 2024 review acknowledges "still limited but encouraging clinical evidence," specifically citing a Phase II trial in ulcerative colitis that showed no toxicity. That is the sum of published human gut data. There are no completed human RCTs showing BPC-157 reduces intestinal permeability, induces remission in IBD, or improves IBS symptoms in people. Earlier trials — documented under designations like PL-10 and PL14736 by the Croatian pharmaceutical company Pliva — examined topical rectal formulations for IBD, but those results remain unpublished in peer-reviewed form at the level of detail needed to evaluate them (Sikiric et al., PubMed 21548867).
Regulatory status is a hard stop here. BPC-157 is NOT FDA-approved and is not a legal dietary supplement in the United States. It is sold as a "research chemical" not intended for human use. The FDA has classified it as a higher-risk Category 2 bulk substance for compounding, citing limited human safety data and potential immunogenicity. WADA has restricted it for competitive athletes.
Actionable takeaway: BPC-157 is legitimate as a research compound with promising animal pharmacology. The tradeoff is that human efficacy has not been demonstrated for gut conditions, and buying it from unregulated vendors means unknown purity and no oversight. Do not treat the rat data as a prescription.
Other Peptides Claimed for Gut Health
KPV: Interesting Mechanism, No Human Data
KPV is a tripeptide (lysine-proline-valine) from the C-terminal end of alpha-melanocyte-stimulating hormone (alpha-MSH). It attracts attention because it appears to travel through the intestinal wall via PepT1, a transporter already busy absorbing dietary di- and tripeptides — which theoretically makes it orally bioavailable without injection.
A 2008 study (PMID 18061177) showed that KPV in drinking water significantly reduced colon inflammation in mice with chemically induced colitis. The mechanism involves NF-kB and MAP kinase inhibition, reducing IL-6, IL-12, TNF-alpha, and IFN-gamma. An earlier paper (PMID 12750433) confirmed KPV's effect is distinct from the melanocortin receptor pathway, making it mechanistically interesting.
The ceiling: all of this is in-vitro cell work and mouse models. KPV is NOT FDA-approved and is not a legal dietary supplement. It is sold as a research chemical not for human use. No human trial has measured its effect on gut permeability, IBD activity, or IBS symptoms. Like BPC-157, the gap between "works in mice" and "works in people" has not been crossed.
Collagen Peptides and Glutathione
Collagen peptides are marketed for gut lining support; the evidence is thin. Glycine, abundant in collagen, has in-vitro barrier properties, but oral collagen supplements have not been shown in well-designed human trials to reduce intestinal permeability. Glutathione peptides face even more skepticism: oral glutathione is extensively broken down in the gut before reaching the intestinal wall.
Where the Human Evidence Is: Real Gut Protocols
This is where the conversation shifts from experimental compounds to interventions with actual trial data.
L-Glutamine
Glutamine is the most abundant amino acid in the bloodstream and the primary fuel source for intestinal epithelial cells. Its role in barrier maintenance is mechanistically solid: enterocytes consume it rapidly to maintain tight junction integrity and produce mucus. The question is whether supplemental glutamine — on top of dietary intake — produces measurable benefits in humans.
A 2024 meta-analysis of 10 RCTs (PMID 39397201) covering 428 adults found that glutamine supplementation did not significantly reduce permeability across all studies combined. However, subgroup analysis told a more specific story: doses above 30 g/day for under two weeks did produce statistically significant reductions in the lactulose/mannitol ratio. Most importantly, the populations where glutamine showed the clearest benefit were critically ill patients and people with specific, established gut pathology.
The clearest human evidence comes from a 2019 RCT published in Gut (PMID 30108163). Researchers enrolled 106 adults with post-infectious IBS-D who had documented intestinal hyperpermeability (confirmed by elevated lactulose/mannitol ratios). Participants received either 5 g of glutamine three times daily or placebo for eight weeks. The primary outcome — a composite reduction in IBS symptom scores — occurred in 79.6% of the glutamine group versus only 5.8% of the placebo group. Intestinal permeability normalized in the glutamine group and did not change in controls. This is an important finding, but with a specific caveat: participants were selected specifically because they had elevated permeability confirmed at baseline. Glutamine's benefit may be concentrated in people who actually have measurable barrier disruption, not in the broader population using it prophylactically.
Actionable takeaway: Glutamine at therapeutic doses (15 g/day or higher) has genuine human RCT support in post-infectious IBS with confirmed hyperpermeability. Using it as a general "gut health supplement" without a confirmed permeability problem is not well supported by the evidence.
Probiotics With Actual RCT Evidence
Certain probiotic strains have a stronger human evidence base for gut barrier support than any peptide currently marketed as a supplement.
Lactobacillus rhamnosus GG (LGG) has been studied for over 30 years. A 2019 review (PMID 30741841) covering multiple RCTs found that LGG consistently reduced antibiotic-associated diarrhea, shortened gastroenteritis duration, and stabilized epithelial tight junctions in cell work. A 2014 human RCT (PMID 24501384) in children with acute gastroenteritis showed LGG supplementation reduced intestinal permeability markers versus placebo. LGG produces biofilm that physically shields the epithelium and modulates local immune response — mechanisms similar to what BPC-157 proponents hope for from peptides. The difference is the human evidence exists.
Actionable takeaway: A well-characterized probiotic strain like LGG, paired with dietary fiber, has a more defensible evidence base than any peptide currently marketed for gut health.
Dietary Fiber and Fermented Foods
This is not the exciting answer, but the data is clear. Dietary fiber feeds short-chain fatty acid (SCFA) producers in the colon; butyrate, the most gut-relevant SCFA, is the primary fuel for colonocytes and essential for maintaining the mucus layer. A 2021 Stanford RCT published in Cell found that a high-fermented-food diet significantly reduced 19 inflammatory protein markers and increased microbiome diversity over 17 weeks — effects a high-fiber diet alone did not match. Fiber and fermented foods have large, replicated human RCTs behind them. The peptides have (at best) Phase II safety signals and animal pharmacology.
How to Think About Gut Health Claims
Mechanistic plausibility is not efficacy. A peptide that blocks NF-kB in a mouse cell line sounds promising. Blocking NF-kB is also a feature of several failed drugs with serious side effect profiles. The gut is not a simple system, and what suppresses inflammation in one context can disrupt immune surveillance in another.
"In clinical trials" is a specific phrase. When BPC-157 papers describe it as "in clinical trials for IBD," they are referring to a Croatian pharmaceutical program from the 2000s that produced Phase II safety data — not a completed Phase III efficacy trial. The gap between Phase II safety and Phase III efficacy is where most drugs fail.
The grey market is not a clinical trial. Self-experimentation with injectable BPC-157 from unregulated peptide labs constitutes anecdote — no standardized dosing, no purity verification, no control group, no systematic outcome tracking.
For anyone managing a chronic gut condition — Crohn's, ulcerative colitis, celiac, or treatment-resistant IBS — the ask is straightforward: consult a gastroenterologist before starting any peptide protocol, and do not reduce prescribed treatment based on internet testimonials.

Frequently Asked Questions
Can I take BPC-157 for gut health? Not legally in the US as a dietary supplement. BPC-157 is sold as a research chemical not approved for human use. The animal data is promising, but no completed human RCT has confirmed efficacy for gut conditions. If you are considering it, discuss with a physician who understands the regulatory and safety landscape — and do not substitute it for diagnosed IBD treatment.
What does "leaky gut" actually mean scientifically? Increased intestinal permeability is a measurable state where the gut barrier lets more substances pass than normal, confirmed via lactulose/mannitol urine tests or blood biomarkers like zonulin. "Leaky gut syndrome" as a diagnostic category is not accepted in mainstream gastroenterology. The underlying mechanism is real; the syndrome framework built around it is not.
Is glutamine worth taking for gut health? Possibly, in specific contexts. The 2019 Gut RCT showed strong effects in post-infectious IBS-D with confirmed permeability problems. Without a confirmed permeability issue, the evidence for routine supplementation is much weaker. Dose matters: studies showing benefit used 15 g/day or more.
Are there any gut-health supplements with real human evidence? Yes — just not the peptides currently marketed for it. Glutamine (technically an amino acid) has the strongest human trial data for barrier support in specific populations. Probiotic strains like LGG have robust RCT data for gut resilience and diarrhea prevention. Strain specificity matters: benefits from one strain do not transfer automatically to another, even in the same species.
Tracking a protocol like this? Our companion app, StackMyMed, lets you log doses, schedule them, and check interactions across everything you take — alongside, never instead of, your clinician’s guidance.
Conclusion: The Bottom Line on Peptides for Gut Health
The gap between "exciting in animals" and "proven in people" defines the peptides-for-gut-health space in 2026. BPC-157 has extensive animal pharmacology — and almost none of that has been replicated in human trials. KPV is mechanistically intriguing and completely unproven in humans. Both are sold as research chemicals with no FDA approval and no purity oversight.
L-glutamine in post-infectious IBS, LGG for gut resilience, dietary fiber for the microbiome — these are less exciting to talk about on social media. They are also legal, well-characterized, and backed by data from actual human beings.
If you have a diagnosed gut condition, that warrants a gastroenterologist, not a research-chemical order. If you are otherwise healthy, the fiber-and-fermented-food approach has a genuine evidence base that no peptide can currently match.
Next steps:
- Learn the fundamentals first: what peptides are and how they work in the body
- Understand the regulatory and safety context: are peptides safe?
- See how peptide research compares in a different use case: peptides for injury recovery
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
