If you are over 50 and considering peptides, here is the honest answer: collagen peptides have real evidence in your age bracket, with randomized controlled trials conducted specifically in sarcopenic older adults showing meaningful gains in fat-free mass and muscle strength when combined with resistance training. GLP-1 receptor agonists — drugs like semaglutide — require physician supervision in this age group because they interact with common medications, alter kidney function thresholds, and can raise fall risk through blood pressure changes. Almost everything else being marketed as "anti-aging peptides" for seniors — BPC-157, growth hormone secretagogues, thymosin-based products sold as supplements — is research-stage at best, unregulated at worst, and in several cases actively concerning when layered on top of the polypharmacy that becomes the norm after 60. This article separates the three categories clearly, so you can make a decision grounded in what the clinical trials actually measured rather than what a wellness website claims.
Summary / Quick Answer: Which Peptides Have Evidence for Older Adults?
The short answer: oral collagen peptides plus resistance training have the strongest RCT evidence for this age group, specifically for muscle mass and strength. GLP-1 drugs are FDA-approved and show similar cardiovascular and glycemic outcomes in adults 65 and older compared with younger patients, but they require physician-supervised prescribing. All other peptides marketed for seniors lack adequate human safety data and carry unresolved drug-interaction risks in a population that is already managing multiple medications.
Best supported by evidence:
- Collagen peptides (15 g/day) plus supervised resistance training for sarcopenia in adults 65+
- Protein at 1.2-1.6 g/kg/day paired with resistance exercise as the muscle-preservation foundation
- FDA-approved GLP-1 agonists prescribed by a physician for type 2 diabetes or obesity-related cardiovascular risk
Not supported by adequate evidence in older adults:
- BPC-157 — no adequate human RCTs
- Ipamorelin, CJC-1295, and growth hormone secretagogues — unapproved, unstudied in seniors, unpredictable drug interactions
- Over-the-counter thymosin alpha-1 — not FDA-approved in the US; human data limited to supervised vaccine-adjuvant studies
Decision shortcut: Before spending money on any peptide product, confirm with your prescriber or pharmacist that it does not interact with your current medication list.
What Changes After 50: Sarcopenia, Immune Senescence, and Recovery
Understanding why older adults have a distinct relationship with peptides requires a brief account of what actually happens to the body after 50.
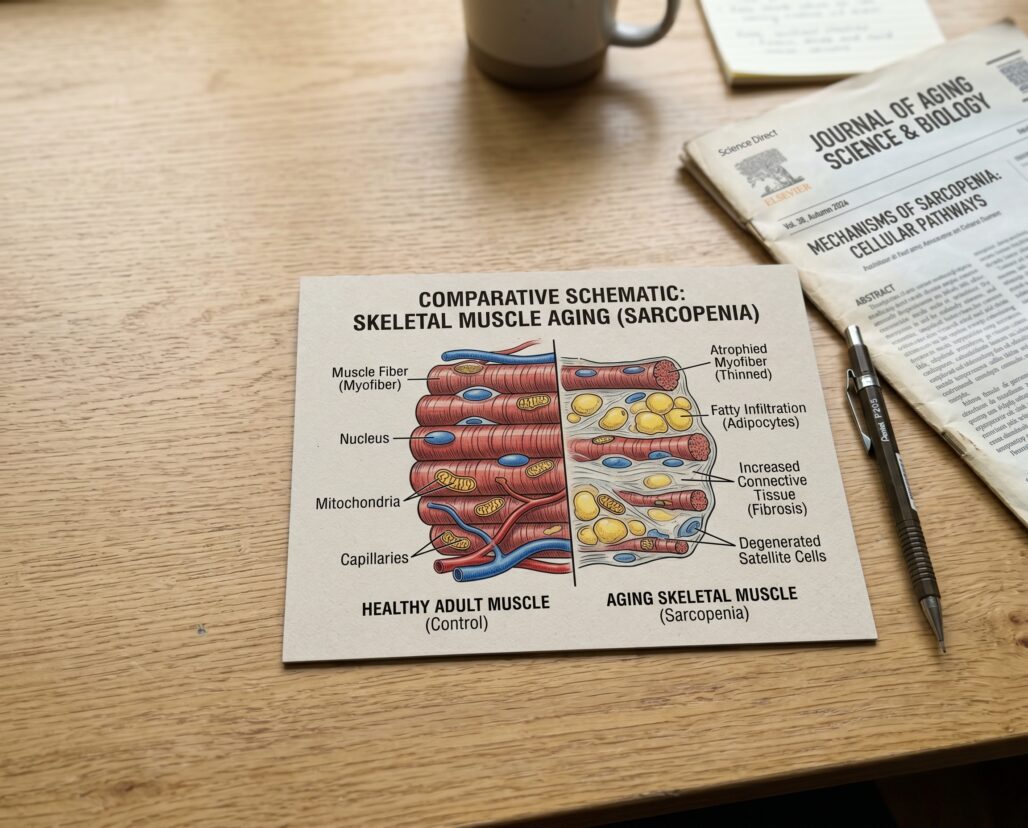
Sarcopenia and dynapenia are the clinical terms for age-related loss of muscle mass and muscle strength, respectively. Strength declines faster than mass in many adults, which is why functional measures like grip strength and gait speed are now part of the diagnostic criteria. Sarcopenia affects an estimated 10-20% of adults over 60 in developed countries and is associated with falls, hospitalization, and loss of independence. Underlying mechanisms include reduced anabolic signaling, impaired protein synthesis efficiency, chronic low-grade inflammation ("inflammaging"), and motor neuron dropout — the targets that collagen peptide and protein supplementation trials are trying to address.
Immune senescence is the age-related decline in immune function that accumulates across decades. The thymus — where T-cells mature — has largely atrophied by the sixth decade of life. This is the biological rationale behind thymosin research: could exogenous thymic peptides restore some of that lost capacity? The evidence suggests a narrow, context-specific answer for vaccine response enhancement. It does not support the broad anti-aging claims appearing on supplement labels.
Recovery and pharmacokinetics change substantially with age. Renal glomerular filtration rate declines roughly 1% per year after 40, so a 70-year-old with no kidney diagnosis may have clearance capacity 30% below their 40-year-old baseline. Hepatic first-pass metabolism also slows. Both changes affect how the body handles any new compound, and polypharmacy — the norm for adults over 65 — multiplies the interaction surface with every added substance.
Collagen Peptides for Older Adults: What the RCTs Actually Show
This is the one peptide category where the evidence in older adults is specific, replicated, and built on trial populations that actually match the demographic.
The landmark study is Zdzieblik and colleagues (2015), a randomized double-blind placebo-controlled trial in the British Journal of Nutrition (PMID 26353786). It enrolled 53 men averaging 72.2 years old with diagnosed Class I or II sarcopenia — clinically documented muscle loss, not a convenience sample. All completed three supervised resistance training sessions per week for 12 weeks. The treatment group received 15 g/day of specific bioactive collagen peptides; the control group received a silica placebo.
Results were statistically significant across all three primary outcomes. Fat-free mass: +4.2 kg (collagen) vs +2.9 kg (placebo), p less than 0.05. Isokinetic quadriceps strength: +16.5 Nm vs +7.3 Nm, p less than 0.05. Fat mass: -5.4 kg vs -3.5 kg, p less than 0.05. No adverse events were reported. The collagen group approximately doubled the strength gain of the placebo group despite both groups doing the same exercise program — a meaningful signal that the protein addition was doing real work.
A broader meta-analysis published in the Journal of Nutrition, Health and Aging (PMID 38350303, 2024) examined 10 RCTs across 1,154 older adults with diagnosed sarcopenia and found that protein supplementation (including whey and collagen) significantly improved appendicular skeletal muscle mass index (standardized mean difference 0.47, 95% CI 0.23-0.71) and gait speed (SMD 1.13, 95% CI 0.82-1.44). The gait speed finding matters for falls risk: adults with gait speeds below 0.8 m/s are at substantially higher falls risk, and improving that number has real-world consequences.
Practical dose guidance from the evidence: The Zdzieblik trial used 15 g/day. Other published trials have used 5-10 g/day with positive outcomes for skin and connective tissue outcomes (which are secondary concerns for many seniors). If muscle mass and strength are the primary goal, the 15 g/day combined with resistance training is the evidence-supported protocol, not a lower dose taken without exercise.
What the evidence does not show for this age group: Collagen peptides have not been shown in older adults to reduce falls (a key outcome for this demographic), reverse cognitive decline, improve bone density, or manage pain from arthritis in isolation. For those outcomes, different clinical pathways exist with their own evidence bases.
GLP-1 Receptor Agonists in Seniors: Real Benefits, Real Supervision Requirements
GLP-1 receptor agonists — semaglutide (Ozempic, Wegovy), liraglutide (Victoza, Saxenda), dulaglutide (Trulicity) — are FDA-approved medications for type 2 diabetes and obesity, not supplements. A post-hoc analysis of the REWIND trial (PMID 33537745, J Clin Endocrinol Metab, 2021) compared dulaglutide outcomes in 5,256 adults aged 65 and older versus 4,645 adults under 65. Major adverse cardiovascular events occurred at similar rates across age groups: 11% vs 13% incidence in older vs younger patients. All-cause mortality, heart failure hospitalization, severe hypoglycemia, and serious GI events were also comparable. The authors concluded dulaglutide had "similar efficacy and safety in patients 65 years and older and those younger than 65 years."
That is reassuring at the population level. But it does not eliminate the specific considerations that make prescriber supervision non-negotiable for seniors using these drugs.
Gastrointestinal effects — nausea, vomiting, diarrhea — are the most common adverse events and are dose-dependent. In older adults, significant GI losses carry higher risk of dehydration-related acute kidney injury, particularly when the person is also taking ACE inhibitors, ARBs, or diuretics — all common in this demographic. The interaction is not theoretical: GLP-1-induced fluid losses can push a compensated kidney into acute injury when renal reserve is already reduced.
Blood pressure and falls risk: GLP-1 agonists produce modest systolic blood pressure reductions (2-4 mmHg in trials). In an older adult already on antihypertensives, this additive effect can tip into orthostatic hypotension, a direct falls precipitant. Reviewing the full medication list with your prescriber before starting is not optional; it is the standard of care.
Renal and hepatic clearance: Your prescriber should account for kidney and liver function before initiating any GLP-1 agonist, and at regular intervals during treatment. Since eGFR naturally declines with age, an older adult with a normal-looking creatinine may still have meaningfully reduced clearance capacity. Dose adjustment or avoidance is required in significant renal impairment.
FDA approval status matters here: Semaglutide, liraglutide, and dulaglutide are FDA-approved drugs dispensed under physician supervision. Compounded versions — which proliferated during supply shortages — are not FDA-approved and have been associated with serious adverse events including hospitalizations. If a GLP-1 agent is the right clinical choice, it should be an approved formulation from a licensed prescriber.
Polypharmacy and Peptide Drug-Interaction Risks
Polypharmacy — five or more concurrent medications — is the norm for adults over 65. Adding any new compound to a stack that already includes ACE inhibitors, statins, beta-blockers, anticoagulants, and diuretics creates potential interaction pathways that are difficult to predict without clinical input.
Three concerns are specific to peptide supplements in this context.
Blood pressure interaction: Peptides marketed with vasodilatory or nitric oxide-boosting claims — BPC-157, certain growth hormone secretagogues — could compound antihypertensive therapy and raise orthostatic hypotension risk. The clinical evidence for these claims in humans is weak, but seniors on blood pressure medications absorb any such effect with less reserve than younger adults.
Anticoagulation risk: Adults on warfarin require stable pharmacokinetics. Most peptide supplements have not been studied for warfarin interaction, and even modest effects on hepatic CYP450 activity can shift INR in either direction — a practical concern for the roughly 10% of adults over 80 living with atrial fibrillation.
The practical rule: Before starting any peptide product, bring the label or compound name to your prescriber or pharmacist and ask specifically about interactions with your current list. This is not bureaucratic caution; it is baseline pharmacological due diligence for a population whose drug clearance has changed.
Thymosin and the Immune Senescence Question
The thymosin research in older adults is worth understanding because it represents a real biological problem with an overstated supplement solution.
Thymosin alpha-1 (Ta1) is approved in several countries (Italy, China) for immune modulation in hepatitis B, hepatitis C, and as a cancer-treatment adjuvant. In the US, it is not FDA-approved for any indication.
The human trial evidence in older adults is narrow and specific. A double-blind placebo-controlled trial (PMID 2642497, 1989) administered injectable Ta1 at 900 micrograms/m2 twice weekly alongside influenza vaccination in men aged 65-99 and found enhanced antibody responses. A 2007 National Institute on Aging review (PMID 17600281) confirmed that vaccine response enhancement had been demonstrated in both animal and human trials, while calling for further study. That is the extent of the senior-specific RCT record: vaccine adjuvant, injectable, supervised, weight-based dosing.
Over-the-counter thymosin supplements are a different product in a different delivery format with no published human data supporting the broader immune claims on their labels. For adults genuinely concerned about immune senescence, the evidence-backed conversation is with a physician about high-dose or adjuvanted influenza vaccines designed for the 65-plus immune profile — those interventions have far more data behind them.
Resistance Training and Protein: The Unglamorous Interventions That Win
No peptide supplement category approaches the evidence base of two unglamorous, unsexy interventions for healthy aging in adults over 50: resistance training and adequate protein intake.
A 2024 meta-analysis (PMID 38350303) across 1,154 sarcopenic older adults found that protein supplementation combined with resistance training improved handgrip strength (SMD 0.67, 95% CI 0.29-1.04) and gait speed (SMD 1.13, 95% CI 0.82-1.44). Those are not laboratory curiosities — gait speed and grip strength predict mortality in this age group with high consistency across independent studies.
Current protein guidance for adults over 60 with sarcopenia risk is 1.2-1.6 g/kg/day, substantially above the 0.8 g/kg recommendation derived from younger populations. Oral collagen peptides fit here as one component of that daily protein total, not as a standalone product. The Zdzieblik 2015 trial worked because both the protein and the exercise load were present.
Resistance training does not require a gym. Resistance band programs, bodyweight progressions, and physiotherapy-led protocols have all produced positive trial outcomes in older adults. The key variable is progressive overload over time, not the equipment. Adults with cardiovascular conditions, osteoporosis, or balance disorders should get medical clearance before starting — not because exercise is dangerous, but because knowing your starting point helps calibrate the load.
For a broader view of how evidence-based longevity strategies compare to peptide marketing, see the peptides for longevity article. For general safety framework, the are peptides safe guide covers regulatory status and adverse event patterns.

FAQ
Are collagen peptides safe for seniors on blood pressure medications?
Published RCTs in older adults have not reported safety concerns with oral collagen peptide supplementation. The 2015 Zdzieblik trial in sarcopenic men averaging 72 years old reported no adverse events across 12 weeks. That said, a 12-week trial result is not a blanket clearance for every medication combination. Check with your prescriber if you are on antihypertensives, anticoagulants, or immunosuppressants before adding any supplement.
Should seniors with kidney disease take collagen peptides?
Collagen peptides are a protein source. Adults with CKD stages 3b-5 are typically on protein-restricted diets, and adding 15 g/day of supplemental protein could breach the ceiling set by their nephrologist. Your prescriber should account for kidney function before any significant change in protein intake. Have that conversation before starting.
Is thymosin alpha-1 available in the US?
Thymosin alpha-1 is not FDA-approved for any indication in the United States and cannot legally be sold as a drug here. Products labeled as "thymosin peptide supplements" lack the safety and efficacy data required for any drug approval. For immune health concerns, speak with your physician about age-appropriate vaccine formulations designed for the over-65 immune profile.
Can peptides help with cognitive decline or dementia?
No peptide is approved by the FDA to prevent, slow, or treat any form of dementia or cognitive decline. If you or a family member are noticing cognitive changes, see a neurologist. Do not delay evaluation or defer diagnosis while trying experimental peptides — some treatable causes of cognitive change (thyroid dysfunction, B12 deficiency, medication effects, normal-pressure hydrocephalus) require timely diagnosis and cannot wait. This is a non-negotiable YMYL caution: an experimental supplement is not a substitute for specialist evaluation.
What about GLP-1 drugs and muscle loss in older adults?
This is a real concern. GLP-1 receptor agonists produce weight loss that includes lean tissue — roughly 25-40% of lost weight can be muscle in trials. For older adults at risk of sarcopenia, that lean mass loss is clinically meaningful. Mitigation strategies include adequate protein intake, maintained resistance training, and regular lean mass monitoring with your prescriber. Some older adults with critically low lean mass reserves may not be good candidates for weight-loss-dose GLP-1 therapy at all. See our article on supplements for GLP-1 muscle loss for more detail.
If you are managing a protocol like this, StackMyMed (our companion app) keeps your doses, timing, and interaction checks in one place. It does not replace medical advice — bring the log to your clinician.
Conclusion: The Bottom Line for Adults Over 50
The peptide landscape looks different when you are over 50. The biological problems being targeted — sarcopenia, immune decline, metabolic risk — are real and clinically significant. But the potential for harm from unvetted supplements is also higher in this age group because of polypharmacy and age-related changes in drug clearance that younger adults simply do not face.
Two categories stand on solid evidence: collagen peptides at 15 g/day combined with resistance training (proven in sarcopenic men averaging 72 years old), and FDA-approved GLP-1 receptor agonists prescribed and monitored by a physician. Everything else marketed as "anti-aging peptides" for seniors lacks adequate human safety data, FDA approval, or both — and carries real potential to interact with the polypharmacy that defines this age group.
The most evidence-supported path is also the least marketable: progressive resistance training, protein at 1.2-1.6 g/kg/day (collagen peptides as one component), and a physician who knows your full medication list. No subscription required. Decades of clinical trial data included.
Next steps:
- What are peptides — grounding in the biology before evaluating specific products
- Are peptides safe — regulatory status and consumer risk framework across categories
- Peptides for longevity — how peptide claims overlap with evidence-based longevity medicine
- Peptides and medications — drug-interaction framework in detail for anyone on multiple prescriptions
This article is for informational purposes and not medical advice. Peptides, especially those marketed for therapeutic use, can interact with medications and health conditions. Consult a licensed physician before starting any supplement, particularly if you are over 65, taking prescription medications, managing chronic kidney or liver disease, or have a history of cardiovascular events. For concerns about cognitive decline, please see a neurologist rather than relying on any supplement intervention.
