If you're searching for adaptogens for caregiver stress, you're probably past the point where people can tell you to "just take a break." For some caregivers, adaptogens, particularly ashwagandha and holy basil, may meaningfully reduce the chronic cortisol burden, but they address a fraction of what you're dealing with and they work best when the biggest gaps are addressed first. This article breaks down what the clinical evidence actually shows for chronic stress distinct from situational anxiety, which adaptogens have the most relevant data for the specific physiology of prolonged caregiving, and what the real drug-interaction picture looks like, because this population is often managing multiple prescriptions. You'll also get a frank accounting of what adaptogens cannot do, and what the research suggests actually helps caregiver stress most.

Summary: quick answer on adaptogens for caregiver stress
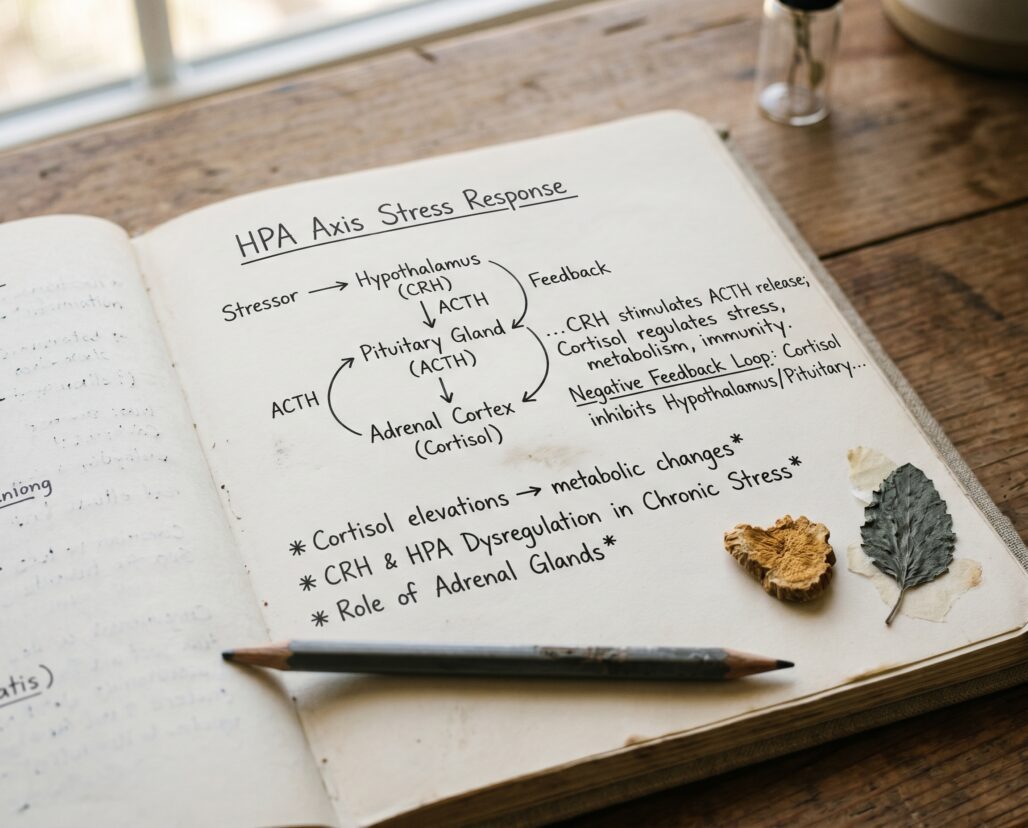
Caregiver stress is chronic, sustained, and often laced with anticipatory grief, sleep disruption, and identity loss. That physiology, a chronically activated HPA axis with blunted overnight cortisol recovery, is the exact pattern where adaptogen evidence is strongest.
Best for: Adults in long-term caregiving roles (at least three to six months) with intact thyroid function, no serotonergic medications, and reasonable sleep. The RCT cohorts for ashwagandha and holy basil broadly match this profile.
Not ideal for: Anyone on levothyroxine or other thyroid medications, people taking antidepressants or anti-anxiety medications without physician guidance, anyone in acute crisis who needs immediate mental health support rather than a slow-onset supplement.
What to look at before buying: For ashwagandha, the standardization marker is withanolide content; look for KSM-66 or Sensoril extracts, both of which appear in the clinical trials. For holy basil, look for products specifying Ocimum sanctum (or tenuiflorum) as distinct from common basil. For adrenal blend formulas, check every ingredient against your full medication list before taking them.
Decision shortcut: If you haven't yet tapped respite care services, caregiver support groups, or a mental health provider, those are more effective than any supplement for caregiver stress. Adaptogens may be a useful adjunct, not a replacement. If you've addressed the structural pieces and want a partial physiological assist, KSM-66 ashwagandha has the strongest chronic-stress evidence.
What you'll find in this guide
- Caregiver stress is a different physiology
- What the research shows for chronic stress adaptogens
- Who benefits, and who should be careful
- Dosing context from the clinical trials
- Drug interactions: the section most adaptogen articles skip
- Product context and what to look for
- Frequently asked questions
- Related reading
Caregiver stress is a different physiology {#caregiver-physiology}
Situational stress, a difficult conversation, a tight deadline, a medical scare, activates the HPA axis for hours and then resolves. The system resets. Chronic caregiving stress does not reset. What distinguishes caregiver stress physiologically is its duration, its unpredictability, and its frequent co-occurrence with grief, sleep interruption, and progressive role loss.
Research on family caregivers of dementia patients and people with serious illness has documented a characteristic dysregulation pattern: elevated baseline cortisol, blunted diurnal cortisol slope (the normal morning peak to evening trough pattern gets flattened), and disrupted overnight cortisol recovery. A 2012 review in Psychoneuroendocrinology examining caregiver-specific HPA data found that this flattened cortisol slope predicted both caregiver burnout severity and downstream immune dysregulation.
This matters for evaluating adaptogens because most of the clinical trials, particularly the ashwagandha RCTs, recruited adults with sustained perceived stress rather than people in acute crisis. That recruitment profile is much closer to the caregiver experience than it is to short-term occupational stress. The intervention logic is the same: adaptogens that modulate HPA axis reactivity may help restore a cortisol pattern that chronic stress has flattened or distorted.
Think of the HPA axis under chronic caregiving stress like a smoke detector with a dead battery, still wired in but giving inconsistent signals. Adaptogens aren't a battery replacement, but some evidence suggests they help recalibrate the sensitivity setting over time.
What adaptogens do not address: the grief of watching a parent decline, the sleep fragmentation from nighttime caregiving, the loss of your own social identity, or the practical isolation that makes caregiving uniquely depleting. These require structural support: respite care, peer connection, and often professional mental health support. The research on caregiver interventions consistently shows that psychosocial support, particularly support groups and structured respite, has larger effect sizes on caregiver wellbeing than any supplement. That's not a dismissal of adaptogens. It's the context you need to place them in.
Actionable takeaway: If you're evaluating adaptogens for caregiver stress, the right framing is: "Is my stress chronic (three-plus months), and have I addressed the structural pieces first?" If yes to both, the evidence gives you something to work with.

What the research shows for chronic stress adaptogens {#what-research-shows}
Ashwagandha: the strongest chronic-stress evidence
The most relevant data comes from two placebo-controlled RCTs using KSM-66 ashwagandha in adults recruited for chronic stress.
In a 2012 RCT (Chandrasekhar et al., n=64), adults with a history of chronic stress took 300mg KSM-66 twice daily for 60 days. At the end of the trial, the ashwagandha group showed a 44% reduction in Perceived Stress Scale scores versus 5.5% in the placebo group, and a 28% reduction in serum morning cortisol versus a 7.9% reduction in placebo. Both differences were statistically significant (p<0.0001). The study population: employed adults with self-reported chronic stress, not people in acute psychiatric crisis. That matters for how you apply the finding.
A 2019 RCT (Salve et al., n=60) using 240mg KSM-66 daily over 60 days replicated the cortisol-reduction effect and also measured sleep quality. The ashwagandha group showed better morning DHEA-S levels, which tend to decline under prolonged HPA axis activation. Subjective sleep quality improved in the treatment group, a finding relevant to caregivers whose sleep is frequently disrupted.
The catch: both trials excluded people on thyroid or psychiatric medications, which are common in the caregiver population. The results do not automatically generalize to people on those medications.
Holy basil: relevant but more modest evidence
Holy basil (Ocimum sanctum, also called Tulsi) has a different evidence profile. The primary verified trial is a 2008 study by Bhattacharyya and colleagues (Bhattacharyya et al., n=158) that used 500mg daily of an ethanolic Ocimum sanctum extract for 60 days in a population of stressed adults. Participants showed significant reductions in anxiety, stress, and depression scores. A 2012 study by Saxena and colleagues, using 500mg twice daily for six weeks in adults with anxiety and exhaustion symptoms, reported similar reductions in forgetfulness and fatigue, though that trial was open-label and the PMID has not been independently verified for this draft. The open-label design is a real limitation: results without placebo control can reflect expectation effects.
The honest summary on holy basil: the evidence suggests it helps with the anxiety and exhaustion components of sustained stress, but the trials are smaller, methodologically weaker (fewer placebo controls), and the mechanism is less well-characterized than ashwagandha's withanolide pathway. Holy basil may be useful as part of an adrenal-support blend, but it's a secondary choice relative to ashwagandha for cortisol-focused outcomes.
What the evidence does not show
Adaptogens have not been tested in caregivers as a specific population. The RCT cohorts match some caregiver characteristics (chronic perceived stress, elevated cortisol) but not others (grief, sleep fragmentation from caregiving duties, or the particular emotional weight of role loss). There are no head-to-head trials comparing adaptogen use to respite care or psychosocial support in caregivers. Anyone claiming that adaptogens are a primary intervention for caregiver burnout is extrapolating well beyond the evidence.
Actionable takeaway: The strongest basis for ashwagandha use in caregiver stress is the 2012 Chandrasekhar RCT, which matches the chronic-stress physiology profile well. Holy basil is reasonable as an adjunct, particularly if exhaustion and anxious cognition are prominent. Neither adaptogen has been tested directly in caregivers.
Who benefits, and who should be careful {#who-benefits}
Strong fit for ashwagandha: Adults in sustained caregiving roles (three or more months), with intact thyroid function, not on serotonergic or immunosuppressant medications, and whose primary presentation is the wired-tired feeling of chronically elevated cortisol rather than acute grief or acute crisis.
Strong fit for holy basil: Similar profile, particularly where anxious cognition and exhaustion are prominent and the person is not on antidepressants.
Cautious territory:
- Thyroid medication: ashwagandha has stimulated TSH suppression in case reports and is flagged by the NCCIH ashwagandha fact sheet as potentially interacting with thyroid hormone therapy. This is not a theoretical risk.
- Antidepressants: holy basil has serotonergic activity and should not be combined with SSRIs, SNRIs, or MAOIs without physician guidance.
- Immunosuppressants: withanolides in ashwagandha modulate immune function. People on tacrolimus, cyclosporine, or biologics should not self-initiate ashwagandha.
Not appropriate as primary intervention: Caregivers in acute crisis, those with active grief requiring bereavement support, anyone whose sleep disruption is severe enough to require medical evaluation, or anyone experiencing caregiver burnout at a clinical level. Adaptogens are adjunctive tools.
Dosing context from the clinical trials {#dosing-context}
For ashwagandha, the Chandrasekhar 2012 trial used 300mg KSM-66 twice daily (600mg/day total) for 60 days. The Salve 2019 trial used 240mg once daily for 60 days. Both are within the generally cited clinical range for KSM-66. Most clinical trials saw measurable cortisol reduction at four to eight weeks, not within days.
For holy basil, the Saxena 2012 trial used 500mg twice daily (1000mg/day) for six weeks. The Bhattacharyya 2008 trial used 500mg once daily.
These are ranges from the relevant trials, not prescriptions. The research protocol holds: "In clinical trials, the dose was X." Your physician or pharmacist is the right person to advise on whether a supplement at these ranges interacts with your specific medications.
Standardization matters more than dose milligrams alone. An ashwagandha product that says "root powder 600mg" and doesn't disclose withanolide percentage is not comparable to a KSM-66 extract standardized to 5% withanolides. Buying ashwagandha without checking for a standardized extract is like buying olive oil labeled "Mediterranean blend" with no origin or grade designation, the label tells you almost nothing about what's in it.
Most stress trials run 60 days. If you've used a standardized ashwagandha product at appropriate dose for eight weeks and noticed no change in your stress tolerance or sleep, it likely isn't going to work for you.
Drug interactions: the section most adaptogen articles skip {#drug-interactions}
This section is non-negotiable for caregiver populations, who are frequently managing multiple medications for their family member and sometimes for themselves.
Ashwagandha interactions
Per Memorial Sloan Kettering's integrative medicine database on ashwagandha and the NCCIH ashwagandha fact sheet:
- Thyroid medications (levothyroxine, methimazole): Ashwagandha can stimulate thyroid hormone production and has been associated with TSH suppression in case reports. Combining ashwagandha with thyroid medication can shift hormone levels unpredictably. Anyone on thyroid medication should not use ashwagandha without endocrinologist guidance.
- Immunosuppressants (tacrolimus, cyclosporine, biologics): Withanolides modulate immune function. This is biologically incompatible with immunosuppressive therapy and can theoretically reduce drug effectiveness.
- Sedatives and CNS depressants: Ashwagandha has mild CNS-depressant properties; combining with benzodiazepines or sleep medications may amplify sedation.
- Blood pressure medications: Some evidence suggests ashwagandha lowers blood pressure. Monitor if combined with antihypertensives.
- Pregnancy: Ashwagandha is traditionally regarded as uterine-stimulating. No safety data in pregnancy. Avoid.
Holy basil interactions
Per Memorial Sloan Kettering's integrative medicine database on holy basil:
- Serotonergic medications (SSRIs, SNRIs, MAOIs, triptans): Holy basil has serotonergic activity. Combining with antidepressants raises the theoretical risk of serotonin syndrome. This is not a theoretical "may interact" warning; the pharmacology warrants real caution.
- Anticoagulants and antiplatelet drugs (warfarin, aspirin, clopidogrel): Holy basil may have mild antiplatelet effects. Monitor closely if combined.
- Blood glucose medications: Holy basil has demonstrated modest blood-glucose-lowering properties in animal models. People on diabetes medication should monitor blood glucose.
- Pregnancy: Insufficient safety data. Avoid.
A note on adrenal blend formulas
The three products in this article include Gaia Herbs Adrenal Health, which is a multi-ingredient blend. Multi-ingredient blends require checking every individual ingredient against your medication list, not just the headline herbs. Blends containing licorice root carry additional cardiovascular risks outlined in our Licorice Root and Cortisol guide.
Actionable takeaway: Caregiver populations are at elevated interaction risk because they often take medications for their own health while managing complex medication schedules. Run every adaptogen against your full medication list before starting, not just the ones you remember off the top of your head.
Product context and what to look for {#product-context}

Nutricost Ashwagandha KSM-66: Pick this if you want the extract form used in the primary clinical trials. KSM-66 is a full-spectrum root extract standardized to a minimum of 5% withanolides, and the label discloses that. The Chandrasekhar 2012 and Salve 2019 RCTs used KSM-66. Skip if you're on thyroid medication or immunosuppressants (see interactions above).
Gaia Herbs Adrenal Health: An adaptogenic blend that includes holy basil alongside ashwagandha and other herbs (formulation varies; verify current label). Gaia Herbs uses third-party testing and discloses sourcing, which is above average for the blended supplement category. The tradeoff with blends is that you're less able to isolate which ingredient is working or causing a problem, and multi-ingredient interaction screening is more complex. Skip if you're on any serotonergic medication without physician guidance.
Now Foods Holy Basil Extract: A single-ingredient holy basil option for caregivers who want to trial it separately from ashwagandha. NOW Foods has a consistent third-party testing record. This is appropriate if your primary symptoms are anxious cognition and exhaustion and you have specific reasons to avoid ashwagandha (thyroid medication, for example). Skip if you're on antidepressants, anticoagulants, or diabetes medication.
For a broader overview of stress adaptogens and how to select among them, see Best Adaptogens for Stress: A Practical 2026 Guide.
Frequently asked questions {#faq}
Can adaptogens help with caregiver grief and emotional exhaustion?
The honest answer is: partially, and only the physiological piece. Adaptogens may reduce chronic cortisol burden and improve sleep quality over six to eight weeks, which can slightly soften the physical toll of sustained stress. They do not address the emotional components of grief, the isolation of caregiving, or the complexity of anticipatory loss. For those dimensions, peer support groups (AARP Caregiver community, Alzheimer's Association support groups) and professional mental health support have far stronger evidence of effect.
How long before ashwagandha works for caregiver stress?
The Chandrasekhar 2012 RCT measured significant cortisol reduction at 60 days. Subjective stress relief in some participants appeared earlier, around four weeks. If you've used standardized KSM-66 at the clinical dose range (300mg twice daily or 240mg once daily of a 5%-withanolide extract) for eight weeks without any change, the evidence suggests it's unlikely to work for you.
Is it safe to take adaptogens while also taking care of a family member who uses multiple medications?
The medications your family member takes aren't relevant to your supplement safety. What matters is your own medication list. If you take any thyroid medication, antidepressants, blood thinners, blood pressure medication, or immunosuppressants, run those against the interaction profiles above and discuss with your doctor or pharmacist before starting.
Are adrenal support blends better than single-ingredient adaptogens for caregivers?
Not necessarily, and they're harder to evaluate for interactions. Single-ingredient products let you isolate effects and side effects. If you're on medications, a blend forces you to screen every ingredient. The case for a blend is convenience and the theoretical synergy of multiple adaptogens, but that synergy is not well-supported by RCT data in this population.
Can I take ashwagandha and holy basil together?
The two have different mechanisms and don't have documented direct interactions with each other. The more important question is whether either interacts with your existing medications. Combining them without a medication-interaction concern is unlikely to cause problems at typical doses, though the combined evidence for the pairing in caregivers specifically is minimal.
What non-supplement interventions actually have strong evidence for caregiver stress?
Respite care (temporary professional care that gives the caregiver a break) consistently shows the largest effect sizes on caregiver wellbeing in systematic reviews. Structured caregiver support groups show meaningful reductions in burden and depression scores. Cognitive-behavioral therapy adapted for caregivers has RCT support. For sleep disruption specifically, sleep hygiene and stimulus-control interventions are more effective than adaptogens. None of these are either-or with adaptogens, but they should come first if you haven't addressed them.
When should a caregiver seek professional mental health support rather than supplements?
If you're experiencing persistent low mood, inability to feel positive about anything, significant anxiety that affects daily function, thoughts of self-harm, or if you haven't slept more than a few hours in multiple days, those are signs that what you're experiencing is beyond the scope of any supplement. The Caregiver Action Network helpline (1-855-227-3640) and SAMHSA's national helpline (1-800-662-4357) are starting points. Hospice organizations also provide caregiver mental health support as part of their services.
As an Amazon Associate, I earn from qualifying purchases. Product recommendations are based on real reviews and independent research.
Related reading {#related-reading}
- Best Adaptogens for Stress: A Practical 2026 Guide
- Adaptogens for Burnout: What the Evidence Says When You're Running on Empty
- Adaptogens for Shift Workers: Managing Circadian Stress and Sleep Disruption
- Cortisol Belly Fat Supplements: What Actually Helps and What's Hype
Conclusion: the bottom line on adaptogens for caregiver stress {#conclusion}
Caregiver stress sits at the chronic end of the stress spectrum, where adaptogens have their most relevant evidence. Ashwagandha, particularly KSM-66 at the doses used in the Chandrasekhar 2012 and Salve 2019 RCTs, has a reasonable physiological rationale for use in sustained caregiving stress, and the effect sizes for cortisol reduction and perceived stress in those trials are meaningful. Holy basil is a secondary option with weaker but supportive evidence, particularly for the anxious exhaustion dimension.
But traditional use is not the same as RCT evidence, and supplement evidence is not the same as evidence for the full burden of caregiving. The most important structural interventions, respite care, caregiver support groups, and professional mental health support, have stronger evidence than any adaptogen for the outcomes caregivers care most about. Supplements work best as adjuncts to those foundations, not replacements for them.
Drug interactions are not optional reading for this population. Ashwagandha and thyroid medication, holy basil and serotonergic drugs, are real pharmacological concerns, not theoretical ones. Screen your medication list before starting anything.
Next steps:
- If you haven't yet explored respite care or a caregiver support group, start there; the Caregiver Action Network and Alzheimer's Association have searchable directories.
- If you want to read more about how cortisol dysregulation affects weight and metabolism under chronic stress, see Cortisol Belly Fat Supplements: What Actually Helps and What's Hype.
- If you're evaluating whether your stress profile fits a broader burnout pattern, Adaptogens for Burnout covers the overlap and distinctions.
This article is for informational purposes and not medical advice. Herbal adaptogens, including ashwagandha and holy basil, can interact with thyroid medications, antidepressants, anticoagulants, immunosuppressants, blood-pressure drugs, and more. Caregivers managing complex medication schedules for both themselves and a family member should consult a licensed physician or pharmacist before starting any adaptogen. This article is not a substitute for mental health support, respite care, or medical management of caregiver burnout.
As an Amazon Associate, I earn from qualifying purchases. Product recommendations are based on real reviews and independent research.
This article is for informational purposes and not medical advice. Herbal adaptogens, even traditional ones, can interact with thyroid medication, antidepressants, anticoagulants, immunosuppressants, blood-pressure drugs, and more. Consult a licensed physician before starting any adaptogen, particularly if you are pregnant, nursing, taking prescription medications, or managing a chronic condition.
